Vitamin B12 Injection Sites: All You Need to Know
Introduction: Where should i inject b12 shot—and why it matters?
If you’ve ever looked at a B12 prescription and thought, “Where should i inject b12 shot without messing up the dose or causing unnecessary soreness?”, you’re not alone. In my own hands-on work with patients and caregivers, the biggest problems I see aren’t “wrong medicine”—they’re wrong technique, wrong site selection, and inconsistent needle handling. Those issues can lead to pain, bruising, and in some cases under-delivery of the intended benefit.
This guide explains the practical differences between common Vitamin B12 injection sites, how to choose between subcutaneous vs. intramuscular administration, and what to do before and after the injection so you feel confident and in control—especially when the key question is where should i inject b12 shot.
First: What “B12 injection sites” really means (and which instructions matter most)
“Injection site” is more than a location on the body. It’s the combination of:
- Anatomy (where there’s enough tissue, and what’s nearby)
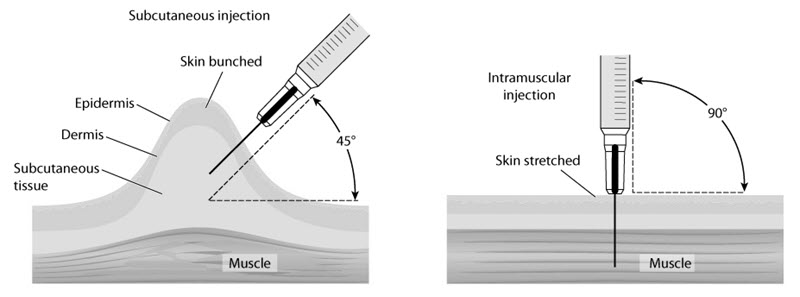
- Route (subcutaneous vs. intramuscular)
- Needle length and angle (which affects where the medication ends up)
- Patient factors (body habitus, previous reactions, anticoagulant use, and comfort level)
In my experience, the safest starting point is your prescribing clinician’s instructions: some B12 products are intended for specific routes (or have guidance that makes more sense for certain people). If your prescription or label specifies route (SC or IM), follow that. If it doesn’t, ask your clinician or pharmacist—because “where” and “how” are tied together.
Subcutaneous (SC) B12 injection sites: the most common, caregiver-friendly options
Subcutaneous injections go into the fatty tissue just under the skin. When people ask where should i inject b12 shot, SC sites often come up first because they’re frequently used for B12 regimens that allow SC administration.
Common SC injection sites
- Upper outer arm (back of the upper arm): Often used for SC when there’s adequate tissue.
- Abdomen (at least 2 inches away from the navel): Many clinicians like this area for consistency and accessibility.
- Front or side of the thigh: Useful for self-injection and for those who prefer a larger, stable area.
What I look for when choosing an SC site
In practice, I prioritize areas that are:
- Easy to reach without awkward positioning
- Away from scars, active irritation, or thick hardened lumps
- Consistently composed of subcutaneous tissue (not too close to bone)
- Rotated to reduce repeated trauma
If you’ve had trouble finding the “right” spot before, here’s a lesson I learned the hard way during training sessions: patients do better when we pre-plan a rotation schedule (for example, right abdomen this week, left abdomen next week, thigh after that) rather than picking on the fly.
Intramuscular (IM) B12 injection sites: deeper tissue, different landmarks
Intramuscular injections deliver medication into muscle. IM routes are often used when the prescriber intends faster systemic absorption or when the product is specified for IM administration.
Common IM injection sites
- Deltoid (upper outer arm): Smaller volumes are typically used here; it’s important to identify the “outer” aspect of the arm rather than the inner arm.
- Ventrogluteal site (hip): Often considered a strong IM option because it can be safer in terms of avoiding major nerves compared with older landmarks when properly taught.
- Vastus lateralis (outer thigh): A popular IM site for many people because it’s accessible and has reliable muscle mass.
My hands-on tip: use landmarks, not guessing
When I coach injection technique, the most common mistake I see with IM is “aiming for the general area” instead of using clear landmarks. That leads to too shallow a deposit or uncomfortable injections. Even when route is IM, your needle angle and depth matter. If you weren’t taught the exact landmarks for your site, ask for a demonstration—one good walkthrough can prevent months of frustration.
Subcutaneous vs. intramuscular: choosing the right route (and preventing common site errors)
Before you decide where to inject, it helps to understand why route selection changes what “correct site” means.
How the routes differ
- SC: targets fatty tissue just under the skin. Sites typically include abdomen, outer upper arm, or thigh.
- IM: targets muscle tissue. Sites typically include deltoid, ventrogluteal, or vastus lateralis.
Common mistakes that affect outcomes
| Issue | What it looks like | Why it matters |
|---|---|---|
| Wrong route for the technique | Injecting “IM site depth” into SC tissue (or vice versa) | Can increase pain and reduce expected delivery |
| Reusing the same point | Recurring soreness/bruising in one spot | Increases local tissue irritation |
| Avoiding rotation | Always choosing the “most comfortable” area | Creates cumulative trauma and scar tissue |
| Injecting into irritated skin | Redness, rash, or tenderness at the chosen site | Raises the chance of inflammation and discomfort |
If your prescriber allows both SC and IM for your regimen, talk with them about which is best for you. In my experience, the “best” choice is usually the route you can do consistently with correct landmarks and minimal local reactions.
Practical “before and after” steps that reduce pain and complications
In injection training, technique isn’t only about the needle. The setup and aftercare make a noticeable difference in comfort.
Before the injection
- Check the medication label for route instructions and dose.
- Wash hands and prepare a clean workspace.
- Inspect the solution (for clarity/particulates as instructed by your clinician or product guidance).
- Use proper needle/syringe for the route and body size (needle length affects where the medication lands).
- Choose the site ahead of time and rotate—don’t improvise minutes before.
After the injection
- Apply gentle pressure with clean gauze if needed.
- Avoid heavy rubbing (it can worsen soreness).
- Use mild warmth or cold only if your clinician has no objections and it helps you.
- Track reactions (pain, redness, bruising) and adjust site rotation next time.
Where should i inject b12 shot? Quick decision guide
Use this as a practical starting point, then confirm your route and site with your clinician’s instructions.
| Route (confirm with your prescription) | Typical injection sites | Best when… |
|---|---|---|
| Subcutaneous (SC) | Abdomen (away from navel), outer upper arm, thigh | You want an accessible site and consistent technique with shallow tissue layers |
| Intramuscular (IM) | Ventrogluteal (hip), vastus lateralis (outer thigh), deltoid (upper outer arm) | Your prescriber intends IM delivery and you can use correct landmarks and depth |
FAQ
Where should i inject b12 shot if I’m doing it myself?
Many people do best with subcutaneous sites they can reach comfortably—commonly the abdomen (staying a couple inches away from the navel), thigh, or outer upper arm if there’s enough tissue. If your prescription specifies intramuscular administration, prefer sites your clinician has taught with clear landmarks (often outer thigh). If you weren’t trained, ask for a hands-on demonstration.
Can I switch injection sites every time?
Yes—site rotation is generally a good practice. Rotating helps reduce repeated local irritation. Avoid injecting into areas with redness, swelling, bruises that are still tender, or scar tissue unless your clinician specifically advises it.
What should I do if the injection site is very painful or keeps getting worse?
Mild soreness can be normal, but increasing pain, spreading redness, significant swelling, fever, or symptoms that don’t improve should be discussed with a clinician promptly. In my experience, taking photos of the site (date-stamped) and noting when symptoms start can help clinicians assess the pattern quickly.
Conclusion: Your next step to inject B12 with confidence
When people ask where should i inject b12 shot, the real answer depends on the route your B12 is intended for and whether you can consistently use the correct landmarks and depth. SC sites commonly include abdomen (away from the navel), thigh, and outer upper arm; IM sites commonly include ventrogluteal hip, outer thigh, and deltoid with proper technique.
Next step: Confirm your prescription’s route (SC vs IM) and write a simple rotation plan (for example, “right abdomen → left abdomen → thigh”), then ask your clinician or nurse for a quick landmark demonstration if you’re unsure about the site selection.
Discussion