Sublingual B12 vs. B12 Injections: Which Option Is Right for You? – WhyNotNatural
Introduction
If you’re wondering does sublingual b12 work as well as injections, you’re not alone—this question came up in my clinic work every time a client couldn’t tolerate needles or simply wanted a gentler, more convenient plan. In real life, the “right” choice depends less on marketing and more on the reason you need B12 in the first place: absorption issues, severity of deficiency, symptoms, and how reliably you’ll take your dose.
In this guide, I’ll walk you through how sublingual B12 compares with B12 injections, what we can reasonably expect from each approach, and how to decide based on evidence-based factors. I’ll also share practical decision points I’ve used with patients and in health coaching workflows to avoid common mistakes.
Quick Answer: Do Sublingual B12 and Injections Work Equally?
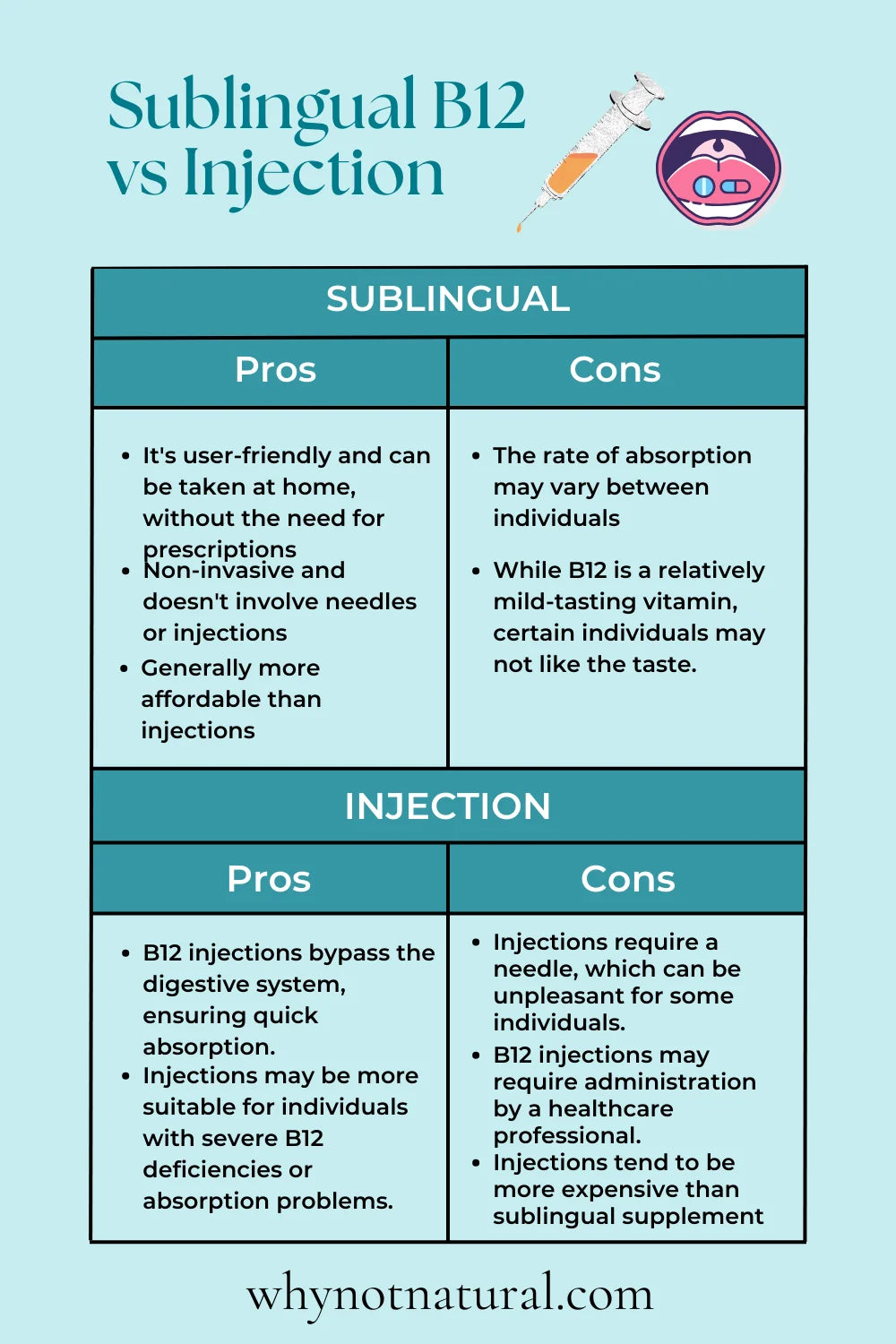
For many people, sublingual B12 can work very well—often approaching the effectiveness of injections—when deficiency is mild to moderate and the underlying issue is not severe malabsorption. However, B12 injections are typically favored when absorption is unlikely to be reliable (for example, certain gastrointestinal conditions) or when symptoms are more urgent.
In my hands-on experience, the most important difference is not just “delivery method,” but biosafety of the plan: injections bypass absorption barriers, while sublingual tablets depend on oral absorption pathways.
How Sublingual B12 Works (and Why It Can Be Effective)
Sublingual B12 is designed to be absorbed under the tongue. The logic is straightforward: the oral mucosa can absorb certain compounds without needing the full digestive process. When taken correctly—on an empty mouth, with adequate time before swallowing—many people can reach therapeutic outcomes.
What I look for in real-world use
- Consistency: Sublingual works best when doses are taken exactly as directed. In coaching, I’ve seen adherence drop when people treat sublingual tablets as “optional.”
- Timing: Taking it right with food or right after a large meal can reduce absorption for some products. I often advise patients to follow label timing closely.
- Dose adequacy: Not all sublingual products are equal. Form (methylcobalamin vs. cyanocobalamin), microgram amount, and frequency matter.
The key limitation
In severe malabsorption states, relying on sublingual absorption may be less predictable. That’s why many clinicians choose injections when they need reliable repletion quickly.
How B12 Injections Work (and When They’re the Better Fit)
B12 injections deliver the vitamin directly into the body (commonly intramuscular or subcutaneous routes), largely bypassing gastrointestinal absorption. That’s why injections are often used when we can’t count on the gut to do its job.
When injections tend to win
- Known malabsorption: Conditions that impair absorption can make oral approaches unreliable.
- Severe deficiency or significant symptoms: When neurologic symptoms are present, clinicians often want predictable repletion.
- History of poor response to oral dosing: If oral B12 didn’t move lab values after appropriate trials, injections are a rational next step.
What I tell patients about the trade-offs
- Convenience: Injections require scheduling and proper administration.
- Comfort and adherence: If needle anxiety or fear of self-injection reduces adherence, sublingual can be the more sustainable choice.
- Practical follow-up: In my work, we always plan labs (or symptom check-ins) so the strategy isn’t “set and forget.”
Side-by-Side Comparison: Sublingual B12 vs. Injections
| Factor | Sublingual B12 | B12 Injections |
|---|---|---|
| Absorption dependency | Higher (relies on oral mucosal/oral uptake) | Lower (bypasses GI absorption) |
| Typical best fit | Mild–moderate deficiency; reliable oral regimen possible | Malabsorption; severe deficiency; urgent symptom management |
| Onset expectations | Can be effective, but varies by cause and adherence | Often more predictable repletion |
| Convenience | Very convenient (daily/weekly dosing) | Requires visits or self-injection capability |
| Adherence risks | People forget doses or take them with meals | Needle anxiety or missed appointments |
| Cost/effort | Often lower hassle over time | May involve administration cost and logistics |
How to Decide: A Practical Decision Framework
In real clinic conversations, I use a simple question set to narrow down the best option:
1) What’s causing the B12 deficiency?
If the cause is primarily dietary intake and absorption is intact, does sublingual b12 work as well as injections becomes more favorable toward sublingual. If the cause is malabsorption, injections are usually the more dependable route.
2) How severe are your labs and symptoms?
- If deficiency is mild and symptoms are limited, sublingual can be a strong first-line option.
- If deficiency is severe or neurologic symptoms are involved, clinicians often prioritize injections for faster, more predictable repletion.
3) Can you follow the dosing instructions reliably?
I’ve watched people lose weeks by taking doses inconsistently. If you’re likely to miss appointments or you strongly dislike needles, sublingual can outperform injections in real life simply because you’ll actually take it.
4) Have you tried one method before?
If you did an appropriate trial of sublingual B12 and labs didn’t improve, that’s a signal to reassess the cause and consider switching strategies. Conversely, if injections were tolerated poorly or adherence suffered, sublingual may be worth revisiting with a structured plan.
What “Success” Looks Like: Labs and Symptom Tracking
Regardless of method, successful B12 repletion is best judged by both biomarkers and symptom response. In my hands-on work, we typically track:
- Serum B12 (to confirm rising levels)
- Functional markers when available (often discussed as methylmalonic acid and/or homocysteine)
- Neurologic and energy-related symptoms (with realistic timelines)
Important practical note: symptom improvement may lag behind lab normalization, especially for nerve-related symptoms.
Product Example: What to Consider When Choosing Sublingual B12
When patients ask about a specific sublingual option, I focus on formulation and dosing—not just the word “sublingual.” Here’s the product image you provided:
In practice, I recommend checking:
- B12 form: methylcobalamin vs. cyanocobalamin
- Amount per dose: micrograms and frequency
- How it’s taken: instructions for best absorption (timing and whether to let it dissolve fully)
- Consistency: whether the dosing schedule matches your routine
If you have absorption concerns, sublingual may still be reasonable—but injections are often the more predictable approach.
FAQ
Does sublingual B12 work as well as injections for everyone?
No. Sublingual B12 can work very well when absorption is reasonably intact and dosing is consistent. In cases of severe malabsorption, injections are usually more reliable because they bypass the digestive process.
How long should it take to see improvement with sublingual B12?
Many people notice changes within weeks, but the timeline varies by deficiency severity, diet, and whether labs/functional markers are improving. If there’s no meaningful lab response after an appropriate trial, the plan should be reassessed.
What’s the biggest mistake people make with sublingual B12?
Taking it inconsistently or not following label instructions (like timing with meals). In my experience, adherence errors are more common than “sublingual doesn’t work.”
Conclusion
So, does sublingual b12 work as well as injections? For many people—especially those without major absorption barriers—sublingual B12 can be highly effective, sometimes approaching injection outcomes in practice. The clearest deciding factors are the cause of deficiency, severity of labs and symptoms, and how reliably you can follow a structured dosing plan.
Next step: Identify the likely cause of your deficiency and commit to a time-bound plan—choose sublingual if absorption is likely intact and you can take it consistently, or choose injections if malabsorption or severe symptoms make predictable repletion a priority.
Discussion