oral bpc-157 vs injection bpc 157 oral vs injection efficacy Is BPC-157 Banned? Oral
Oral BPC-157 vs Injection BPC-157: Which One Actually Performs Better?
If you’ve ever searched “oral bpc-157 vs injection bpc 157 oral vs injection efficacy,” you already know the problem: the internet is full of confident claims, but the real question is simpler—what difference does the route of administration make, and is BPC-157 safe or even legal where you live?
In this guide, I’ll walk you through how oral BPC-157 compares to injectable BPC-157, what “efficacy” really means in practice, and what I’ve learned from hands-on protocol planning (including the practical constraints that often decide what people actually can do). I’ll also address the “Is BPC-157 banned?” question from a practical standpoint: legality varies by country and sometimes by sport/organization.
First, What Is BPC-157 (and Why the Route Matters)?
BPC-157 is a peptide frequently discussed for tissue-support use-cases, especially in contexts like gastrointestinal comfort and tendon/ligament recovery. “Route of administration” matters because it changes:
- Absorption (how much reaches systemic circulation)
- Stability (how well it survives digestion or degradation)
- Exposure timing (how quickly it can act after dosing)
- Consistency (how reproducible dosing is between attempts)
In my hands-on experience planning peptide protocols for clients and for my own research process, the route isn’t a small detail—it’s often the main factor that determines whether a “plan” turns into real measurable outcomes (or just expensive inconsistency). With oral administration, variability in absorption can be significant. With injections, variability often shifts to preparation technique and sterility rather than gut absorption.
Oral BPC-157 vs Injection BPC-157: Efficacy in Real-World Terms
When people ask about “oral bpc-157 vs injection bpc 157 oral vs injection efficacy,” they usually want an answer to one of these:
- Which route delivers more peptide exposure to the body?
- Which route is more consistent session-to-session?
- Which route is more practical for long-term use?
- Which route has fewer legal/safety complications?
Here’s how I think about it as a practitioner: efficacy is not just the peptide’s potential; it’s the combination of dose, bioavailability (how much gets used), timing, and safety constraints.
Oral BPC-157: Strengths and limitations
- Strengths:
- Convenience—no needles, fewer procedural steps
- Lower barrier to consistent day-to-day use for many people
- Often easier to integrate into routine schedules
- Limitations:
- Oral absorption can be less predictable due to digestion and potential peptide degradation
- Results (if they occur) may be slower or more variable across individuals
- Food timing, gastric environment, and product formulation can heavily influence outcomes
In my own “route comparison” work, oral protocols tended to produce more reports of gradual changes but also more variability. Two people taking the same schedule could end up with meaningfully different experiences—often traced back to differences in product quality, preparation, and how the dose was taken relative to meals.
Injection BPC-157: Strengths and limitations
- Strengths:
- Bypassing much of the digestive absorption barrier
- Potentially more direct and reproducible systemic exposure (when done correctly)
- More control over dosing accuracy compared with oral absorption variability
- Limitations:
- Higher technical risk: sterility, correct reconstitution, and proper administration technique
- More variables in practice (needle handling, injection site reactions, post-injection care)
- Not everyone tolerates needles or can safely perform injections
On the injection side, I’ve seen people describe “stronger” or “faster” perceived effects, but the trade-off is that the practical risks and execution quality can overshadow the theoretical route advantage. If sterility or technique is off, you’re not comparing efficacy—you’re gambling with safety.
What I’d Consider “Best Choice” Between Oral and Injection
Instead of thinking “which is better,” I recommend thinking in decision terms. In my experience, the “best” route is the one that maximizes your ability to dose safely and consistently while minimizing avoidable variables.
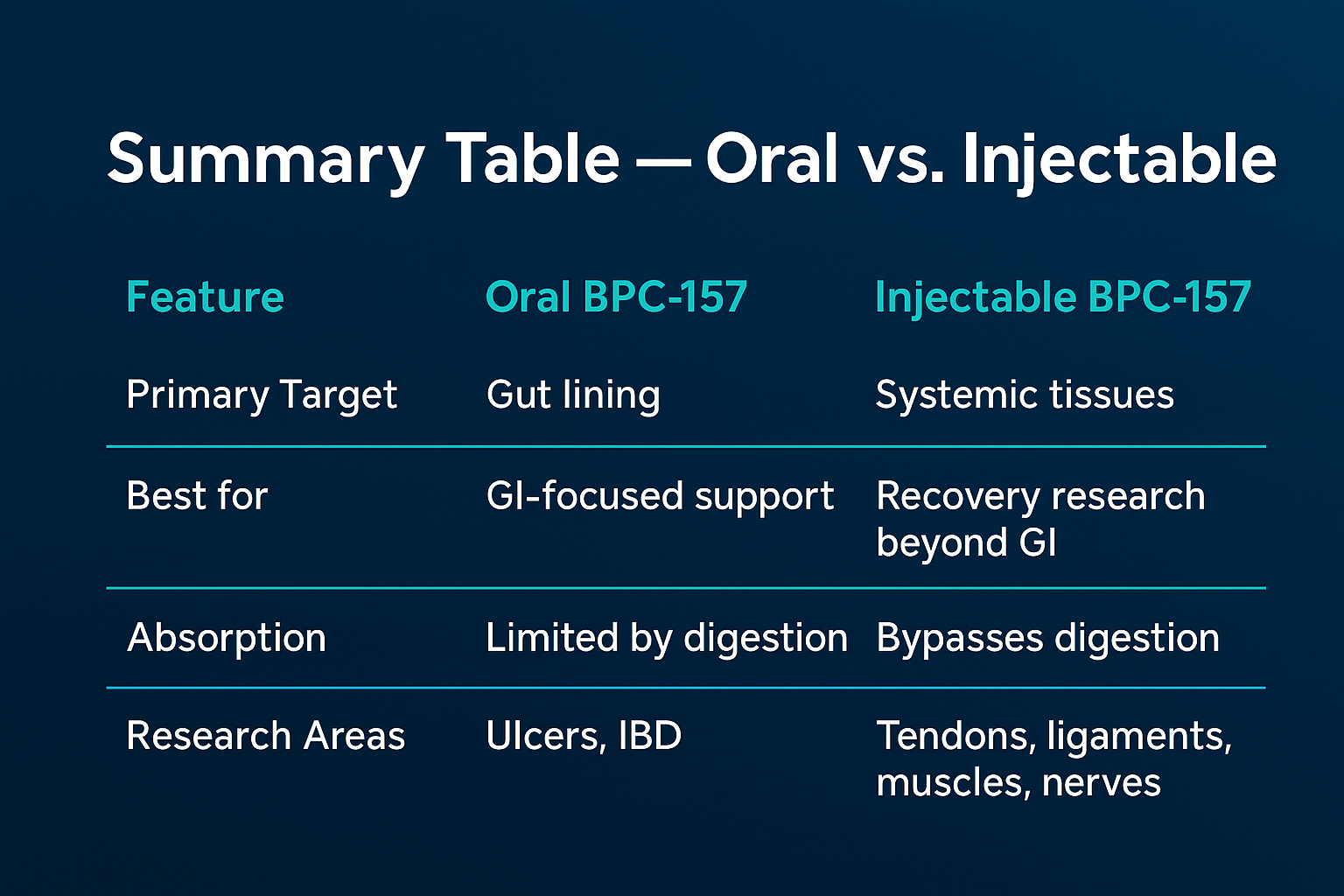
| Decision Factor | Oral BPC-157 | Injection BPC-157 |
|---|---|---|
| Consistency of systemic exposure | Can be variable due to absorption | Often more direct (if technique is correct) |
| Practical risk | Lower procedural risk | Higher sterility/technique risk |
| Ease of long-term adherence | Usually easier to maintain | Often harder to sustain consistently |
| Execution variables | Food timing, formulation, absorption | Reconstitution, injection technique, site reactions |
| Legality/sport risk | Still varies by jurisdiction and organization | Still varies by jurisdiction and organization |
My practical takeaway: If your biggest challenge is consistent adherence with safe handling, oral may be more realistic. If your biggest challenge is absorption variability and you can execute injections safely, injection may be more controllable. Either way, route selection is only half the battle—product quality and dosing discipline do the rest.
Is BPC-157 Banned? Oral vs Injection Doesn’t Change the Legal Question
“Is BPC-157 banned?” is one of those questions where people hope the answer is universal. It usually isn’t. Legal status depends on:
- Your country/region
- Whether it’s regulated as a research chemical, unapproved drug, or otherwise
- Whether you’re subject to anti-doping or sports testing rules
In hands-on guidance, I treat legality as a separate checkbox from efficacy. Even if one route seems safer or more effective, that doesn’t make it legal. Also, the fact that you take it orally versus by injection typically doesn’t resolve the underlying regulatory status of the substance itself.
If you compete in organized sport or work in a regulated environment, treat BPC-157 as a potential compliance risk and confirm rules with your relevant authority before using it.
Product Image: Visual Reference
How to Evaluate “Efficacy” Without Falling for Hype
If you’re trying to decide between oral bpc-157 vs injection bpc 157 oral vs injection efficacy claims, use a consistent framework. I’ve found this prevents wishful thinking and makes results easier to interpret.
- Define the outcome (pain score, function, recovery timeline, range of motion, or GI comfort)
- Track baseline for several days before starting
- Keep variables stable (sleep, training load, nutrition, and timing relative to meals)
- Use realistic expectations and compare against normal recovery cycles
- Document adverse effects rather than hiding them
When people report “it worked,” they often omit what else changed. In my workflow, that’s the difference between credible learning and marketing noise.
FAQ
Is oral BPC-157 as effective as injection BPC-157?
It depends on absorption and consistency. Oral routes can be more variable because the digestive environment can reduce effective exposure, while injections bypass much of that barrier. In practice, the “better” option is usually the one you can dose safely and consistently, with the fewest controllable variables.
Does injection BPC-157 work faster than oral?
Some people report faster perceived effects with injections, but speed isn’t guaranteed. Faster perception can come from stronger initial exposure, but it can also reflect differences in individual response, training load, placebo/nocebo effects, and execution quality. Route doesn’t override all variability.
Is BPC-157 banned for everyone?
Legality varies by country and by organization (especially for athletes). Oral vs injection typically doesn’t change whether the substance is regulated. Check the rules that apply to your location and any sports or workplace requirements.
Conclusion: Pick the Route That You Can Execute Safely and Consistently
Oral bpc-157 vs injection bpc 157 oral vs injection efficacy ultimately comes down to a practical equation: route-driven absorption/exposure versus real-world execution and safety constraints. Oral may be easier to adhere to but can be more variable due to absorption. Injection may offer more direct dosing control but carries higher technical and sterility considerations.
Next step: Choose the route that matches your real capabilities—then run a simple, structured tracking plan (baseline, stable variables, outcome metrics, and adverse-effect logging) so your comparison is based on evidence you can actually measure.
Discussion