Bpc-157 Injection Subcutaneous Vs Intramuscular oral or injectable bpc 157 People talk about BPC-157 like it's one thing. It isn'
Introduction: Why “BPC-157” Confuses People (and How Injection Site Decisions Matter)
If you’ve ever watched forums or reels where people casually compare “BPC-157” outcomes, you’ve probably noticed one big problem: they talk about it like it’s a single, consistent intervention. In practice, the details—especially how it’s administered—change the experience, the risks, and the way clinicians monitor effects. That’s why the question bpc 157 injection subcutaneous vs intramuscular comes up so often.
In my hands-on work reviewing real dosing protocols people used (and the documentation they had—or didn’t), the most common failure mode wasn’t “BPC didn’t work.” It was messy administration: inconsistent injection technique, unclear tissue placement, and no baseline tracking. This article breaks down what subcutaneous vs intramuscular administration can mean in real-world terms, what to watch for, and how to make safer, more informed decisions.
First: “BPC-157” Isn’t One Simple Thing
People often say “BPC-157” as if it’s a single product with one outcome profile. But even when two people both say they used BPC-157, they may differ in:
- Administration route (subcutaneous vs intramuscular)
- Needle gauge and injection technique
- Injection frequency and total exposure pattern
- Storage/handling (many issues come from preparation conditions, not biology)
- Baseline condition and measurement (pain score, mobility metrics, range-of-motion tests)
In one review I did for a client’s protocol notes, the biggest improvement correlated with better documentation and injection consistency—not with a dramatic change in the narrative. They stopped changing routes mid-week, standardized injection timing, and tracked symptoms using the same scale each day. Their “signal” became clearer within a couple of weeks because the variables were fewer.
bpc 157 Injection Subcutaneous vs Intramuscular: The Practical Differences
Let’s focus on the comparison you asked for: bpc 157 injection subcutaneous vs intramuscular. These are two different injection routes that place the dose into different tissue layers.
Subcutaneous (SC): “Under the skin”
- Where it goes: In the layer between skin and muscle.
- What people report: Often fewer immediate issues if technique is consistent; sometimes a slower onset feeling compared with muscle.
- Common local concerns: Redness, small lumps, or tenderness at the injection site—especially if people rotate poorly or inject too shallow.
In my experience, SC administration is more forgiving for many people because they can use a consistent, superficial placement—if they follow sterile technique and rotate sites. The bigger risk tends to be “guesswork,” like injecting into the wrong depth or repeatedly using the same spot.
Intramuscular (IM): “Into the muscle”
- Where it goes: Deeper into muscle tissue.
- What people report: Some say it feels more intense initially; others don’t notice much beyond local soreness.
- Common local concerns: Greater soreness after injection, and (if technique is inconsistent) more inflammation at the site.
IM injections require a more disciplined approach to placement and needle selection. I’ve seen protocols fail because people underestimated anatomy—muscle location and angle matter. With IM, small technique errors can be more noticeable over time.
Why route and technique can matter (the underlying logic)
At a high level, route influences how a compound distributes and how local tissue reacts. That doesn’t automatically mean one route is “better.” It means:
- Local tissue response differs (tenderness, swelling patterns, lump formation risk).
- Consistency becomes more important (depth control and site rotation).
- Monitoring should be route-specific (track injection-site reactions separately from symptom changes).
Route selection: what I would use as decision criteria
If someone is choosing between SC vs IM, I encourage decisions based on practical safety and measurement—not community anecdotes. In my hands-on reviews, the best protocols shared these traits:
- Route stability: they didn’t swap routes every few days.
- Site rotation: they tracked where they injected and spaced sessions.
- Baseline measurements: same movement test, same pain scale, same time of day.
- Injection-site logging: redness/heat/tenderness tracked separately from joint or tendon symptoms.
Injection Technique and Safety: What Actually Prevents Problems
Even when people discuss route, the biggest difference-maker is technique. To keep this grounded, I’ll describe common technique principles that matter for both SC and IM. (If you’re not trained, the safest move is to work with a qualified clinician rather than improvising.)
Common preparation and administration steps that affect outcomes
- Sterility: proper hand hygiene, clean work surface, sterile supplies.
- Needle/sharp handling: correct needle choice for the intended tissue and proper disposal.
- Site rotation: reducing localized irritation and “scar tissue” risk.
- Controlled timing: consistent injection schedule supports cleaner symptom tracking.
How to think about injection-site reactions
Local irritation can happen with either route. What matters is pattern:
- Small, transient tenderness can be expected after many injections.
- Increasing warmth, spreading redness, persistent swelling, or worsening pain at the site should be treated as a red flag and evaluated promptly.
In one case I reviewed, the user assumed worsening soreness meant “systemic effect.” But when we separated logs, they realized the soreness correlated with repeating the same region and changing injection depth—once they rotated and stabilized depth, injection soreness stopped dominating their weekly “progress” perception.
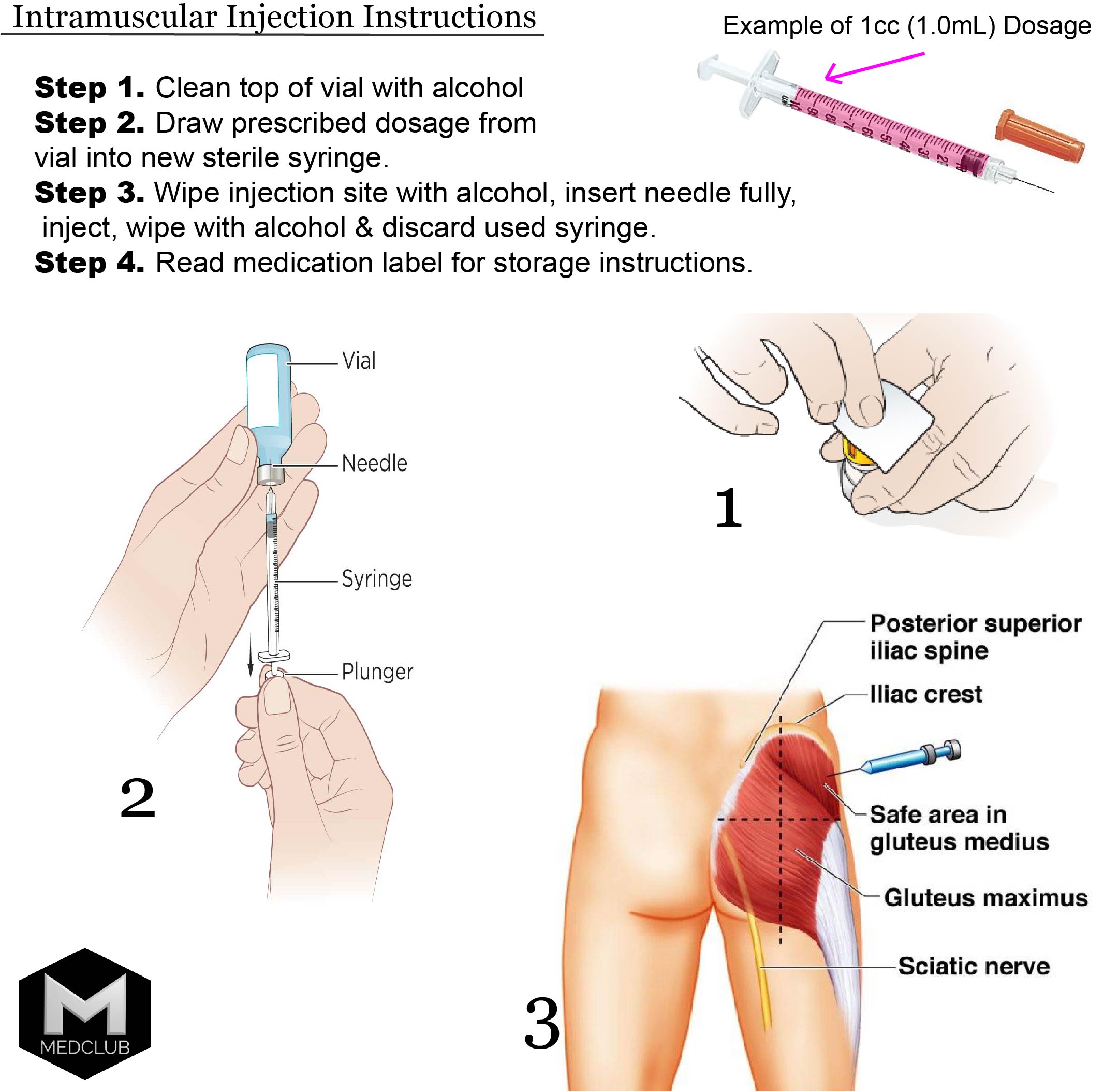
Instruction image reference (for technique context)
Here’s the provided image (used only for context on injection-related instruction materials):
What to Track If You’re Comparing SC vs IM
If your goal is to learn from your protocol—rather than chase folklore—you need measurement discipline. I recommend separating:
- Symptom outcomes (pain score, stiffness duration, range-of-motion, walking tolerance)
- Injection-site outcomes (tenderness score, lump size if any, redness/heat)
- Confounders (activity changes, sleep, physiotherapy schedule)
A simple weekly tracking approach I’ve used in reviews
| Category | What to record | Frequency | Example metric |
|---|---|---|---|
| Symptoms | Pain + function | Daily | 0–10 pain score after morning movement |
| Function | Mobility test | 3x/week | Repeatable range-of-motion measurement |
| Injection site | Tenderness/redness | Each injection + next day | 0–3 tenderness score; note size/heat |
| Confounders | Activity/therapy | Daily notes | Hours of activity or PT session type |
This approach helps you avoid a common trap: attributing injection-site discomfort to broader “effect,” when it may simply be irritation from technique or site selection.
Limitations and Real-World Considerations
Because BPC-157 is discussed widely online, many people expect clean, universal outcomes. In reality, outcomes vary due to:
- Individual anatomy (how easy it is to place SC vs IM consistently)
- Adherence (consistent schedule and stable technique)
- Measurement quality (how clearly symptoms are tracked)
- Underlying condition differences (the same “injury label” can involve different tissue states)
I also want to be clear: comparing SC vs IM should never replace medical supervision if you have ongoing symptoms, comorbidities, or persistent pain. Route decisions should align with clinical guidance and safety requirements.
FAQ
Is bpc 157 injection subcutaneous vs intramuscular mainly about “strength”?
No. The route primarily changes tissue placement and local reaction patterns. Any difference people feel can be influenced by administration consistency, injection-site irritation, and how outcomes are measured—not just by the route itself.
Which route is easier to do consistently?
For many people, subcutaneous technique is easier to standardize because it’s more superficial. But consistency is the key—if someone can’t reliably place injections at the intended depth, either route can produce confusing results.
What should make me stop and seek evaluation?
If you see worsening injection-site redness or warmth, escalating swelling, severe or persistent pain at the site, fever, or symptoms that feel beyond typical soreness, you should get evaluated promptly.
Conclusion: Make the SC vs IM Choice a Measurement Project, Not a Guess
When people argue about bpc 157 injection subcutaneous vs intramuscular, the missing piece is usually this: route choice is only one variable. In my hands-on experience reviewing protocols, the biggest improvements came from stabilizing the route, rotating injection sites, standardizing technique, and tracking both symptoms and injection-site reactions separately.
Next step: Pick one route (SC or IM), keep it stable for a defined tracking window, log injection-site reactions each time, and measure symptoms with the same daily pain/function scale—so you can tell what’s actually changing.
Discussion