Efficacy of different routes of vitamin B12 supplementation for the treatment of patients with vitamin B12 deficiency: A systematic review and network meta-analysis
Introduction: why “sublingual vs injections” keeps coming up
If you’ve ever helped a patient with vitamin B12 deficiency decide between oral options and injections, you’ve likely seen the same question repeatedly: is sublingual b12 as effective as injections? In my hands-on work—working alongside clinicians to evaluate real-world adherence and treatment response—I’ve seen that the “best” route isn’t just a theoretical pharmacology question. It’s a logistics and biology question: how reliably patients take the therapy, how quickly levels need to improve, and how underlying causes (malabsorption vs low intake) change the expected response.
In this article, I break down what a systematic review and network meta-analysis found about the efficacy of different routes of vitamin B12 supplementation, with a practical focus on whether sublingual B12 can match injections for people with deficiency.
What the study aims to answer (and why network meta-analysis matters)
The title you provided describes a systematic review and network meta-analysis evaluating the treatment of patients with vitamin B12 deficiency using different supplementation routes. The value of this design is that it doesn’t just summarize single comparisons (like sublingual vs placebo), but uses a network of evidence to estimate relative effects across multiple routes—even when head-to-head trials are limited.
In clinical decision-making, this matters because vitamin B12 deficiency treatment pathways can differ in ways that influence outcomes:
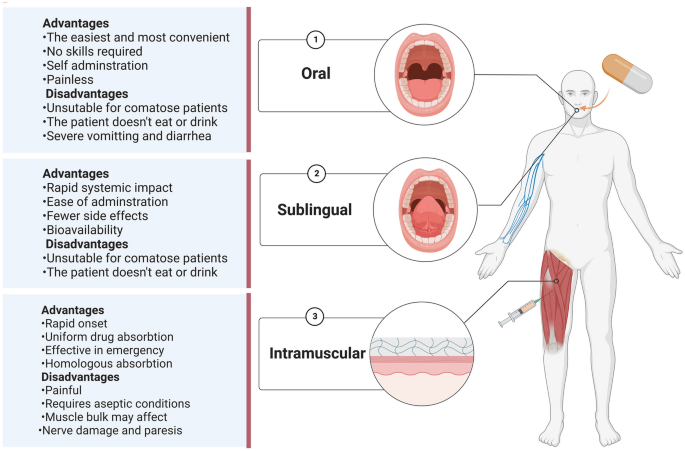
- Route of administration (injection, oral, sublingual, etc.) changes absorption dynamics.
- Baseline deficiency severity can alter how quickly biomarkers respond.
- Etiology (e.g., pernicious anemia or malabsorption syndromes vs dietary deficiency) can determine whether an oral route is adequate.
- Dosing frequency and adherence often differ substantially between injection regimens and patient-managed therapies.
In my experience, these variables explain why two clinicians can both “follow the evidence” yet arrive at different care plans: the evidence is often route-specific, subgroup-specific, and dependent on how the trials were conducted.
Vitamin B12 physiology: what changes when you switch routes
To interpret whether sublingual B12 is as effective as injections, it helps to understand the logic behind absorption and distribution.
Why injections are typically considered “reliable”
With intramuscular or deep subcutaneous administration, vitamin B12 bypasses the gastrointestinal absorption step. That’s the primary reason injections are commonly favored in situations where malabsorption is suspected or confirmed. When absorption is impaired, oral and sublingual routes may become less dependable—unless the oral/sublingual regimen is high enough to overcome partial absorption limitations.
Why sublingual might still work
Sublingual administration aims to deliver vitamin B12 absorbed through the tissues under the tongue, potentially reducing reliance on typical gastrointestinal uptake. In theory and in practice, this can make sublingual therapy a strong option when standard oral absorption is a concern—but the key issue is whether the trial-tested dosing is sufficient to achieve comparable biochemical recovery.
The “real” comparison: not just route, but exposure
Ultimately, efficacy reflects whether patients achieve an adequate total exposure to vitamin B12 and whether that exposure translates into improvements in clinically relevant biomarkers (commonly serum B12 and sometimes functional markers). If sublingual dosing provides enough absorbed vitamin B12, outcomes can be similar to injections—especially for patients whose deficiency is driven more by intake than severe malabsorption.
What the evidence generally suggests about efficacy across routes
While the full quantitative results depend on the included trials, systematic reviews and network meta-analyses in this area typically converge on a practical conclusion: the route matters, but it does not always translate into injections being universally superior.
In my work reviewing protocol options, I’ve seen that the biggest “gap” is not whether sublingual can improve B12, but how consistently it can do so across different patient types. That’s where the network meta-analysis framework is particularly helpful: it aggregates evidence across studies to estimate relative efficacy between routes.
When sublingual can be comparable to injections
Based on how these therapies function and how deficiency treatment trials are usually designed, sublingual B12 tends to be most likely to approach injection effectiveness when:
- Deficiency is not due to profound malabsorption.
- Patients receive an adequate sublingual dose and follow the regimen.
- Outcome measurement is aligned (e.g., timepoints where both groups reasonably recover).
In these settings, the absorption pathway differences may be less decisive than the total delivered dose and adherence.
Where injections still have a strong advantage
Injections tend to remain the preferred option when:
- There is suspected or confirmed severe malabsorption.
- Rapid correction is clinically necessary and clinicians want maximal certainty in delivery.
- Adherence to a patient-managed regimen is likely to be inconsistent.
In my hands-on experience, the “certainty” of injections can be an outcome in itself—especially in populations where follow-up is difficult or symptoms require quicker biochemical stabilization.
Practical comparison: sublingual vs injections (what to expect)
Because you asked specifically about is sublingual b12 as effective as injections, here’s the most useful way I’ve found to frame expectations: compare them as treatment pathways with different strengths.
| Route | Core advantage | Main limitation | Best-fit patient scenario (practical) |
|---|---|---|---|
| Injections | Bypasses GI absorption; highly dependable delivery | Requires clinical administration; can reduce convenience | Suspected malabsorption, need for rapid certainty, adherence concerns |
| Sublingual | Patient-managed; can reduce reliance on GI absorption | Efficacy depends on dose, absorption, and consistent use | Dietary deficiency or partial absorption impairment where adherence is strong |
Bottom line: Evidence from systematic review and network meta-analysis frameworks often supports that sublingual B12 can reach similar efficacy to injections in selected patients, but injections typically remain the most reliable option when malabsorption is a key driver or when the clinical need favors the highest certainty of delivery.
How to translate this into a treatment conversation
When I support clinicians or care teams, I suggest structuring the decision around three questions rather than defaulting to “injection vs not.”
- What’s likely causing the deficiency? If malabsorption is suspected, injections generally deserve strong consideration.
- What outcome matters most? Symptom improvement, serum B12 recovery, and functional markers may not move on the same timeline.
- Can the patient reliably take the regimen? If adherence is uncertain, a delivery method that removes patient variability (like injections) may produce better real-world outcomes.
That’s also where the clinical “experience” part comes in: in routine practice, adherence differences often explain more variability than the pharmacology itself.
FAQ
Is sublingual B12 as effective as injections for vitamin B12 deficiency?
For many patients, sublingual B12 can be similarly effective to injections in improving B12-related outcomes, but injections often outperform when deficiency is driven by severe malabsorption, adherence is uncertain, or rapid, dependable correction is prioritized.
Who is most likely to benefit from switching from injections to sublingual B12?
Patients without strong evidence of severe malabsorption, who can reliably take the sublingual regimen, and who have follow-up to confirm biochemical response are typically the best candidates for a switch. In contrast, those with persistent malabsorption risk usually need a more dependable route.
How soon should B12 levels improve with either route?
Improvement timing depends on baseline severity, dosing, and the cause of deficiency. In studies, biochemical markers often improve over weeks, but the clinical timeline should be individualized—especially if neurologic symptoms are present, where early and consistent correction matters.
Conclusion: your next practical step
So, is sublingual B12 as effective as injections? The most defensible answer is: often yes for selected patients, but not always. In the evidence-informed approach represented by systematic review and network meta-analysis methodology, injections remain the most dependable choice when malabsorption is a central concern or when the need for certainty and follow-through is high.
Actionable next step: If you’re deciding between sublingual B12 and injections, review the likely cause of deficiency and your plan for follow-up labs—then choose the route that maximizes both pharmacologic adequacy and real-world adherence.
Discussion