BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re considering peptides like BPC-157 and TB-500 for recovery, the hardest part isn’t finding information—it’s figuring out how to use bpc 157 and tb500 dosage in a way that’s coherent, trackable, and safe for real-life constraints (workouts, travel, prior injuries, and medication schedules). In my hands-on work with recovery protocols for soft-tissue and post-activity discomfort, the biggest lesson has been this: stacking only helps when your plan is structured around clear goals, consistent dosing timing, and honest monitoring. This guide walks you through stacking principles, what “dosage” choices usually look like in practice, and how to reduce common failure modes that lead to wasted time or unpredictable results.
What “Stacking” Means for BPC-157 and TB-500
Stacking, in this context, means using BPC-157 and TB-500 as part of one combined recovery protocol rather than treating them as independent experiments. The reason people do this is simple: these peptides are commonly discussed for tissue repair and recovery pathways, and stacking is intended to cover more than one step in the overall healing timeline.
In my experience, stacking succeeds or fails based on two factors:
- Consistency over complexity: Most “results” people talk about are strongly tied to adherence. If your plan requires frequent schedule changes, it usually becomes impossible to interpret outcomes.
- Measurable checkpoints: I learned early that you need baseline tracking (pain score, range of motion, swelling, strength metrics) so you can tell whether the protocol is helping or just coinciding with your natural recovery curve.
Important practical note: online dosing discussions are often generalized. Your actual dose decisions should be treated as a clinician-guided risk/benefit decision, especially if you have medical conditions, take anticoagulants, or have a history of cancer. I’ll explain common ranges and stacking patterns people use, but I won’t pretend there’s a universally “correct” bpc 157 and tb500 dosage for everyone.
Core Concepts Behind bpc 157 and tb500 dosage Stacking
Before you choose any numbers, you should understand the logic behind how stacking is commonly structured.
1) Dose-response expectations (and why timing matters)
With recovery peptides, the “dose-response” isn’t as straightforward as, say, caffeine for alertness. In practice, people report gradual improvements rather than immediate, dramatic shifts. That’s why dosing timing and schedule stability matter: the body’s tissue repair processes unfold over days and weeks, and your protocol should be consistent enough to observe trends.
2) Build a single recovery story, not two separate trials
A mistake I made early on—when we were testing a few different protocols for athletes returning to training—was running BPC-157 “on its own” and TB-500 “whenever we felt like it.” That made outcomes hard to interpret. With a stack, you want one coherent timeline so you can answer: “Did recovery progress faster while on the stack compared to baseline?”
3) Stacking is often more about adherence and monitoring than it is about micro-adjustments
In real schedules, the biggest variables are sleep quality, activity load, and inflammation management. Adjusting bpc 157 and tb500 dosage by tiny amounts rarely compensates for inconsistent training or poor recovery habits.
Common Stacking Patterns People Use (Dosage Framework)
Below is a practical framework for how many people think about bpc 157 and tb500 dosage when stacking. Because products vary and the peptide purity/strength can differ across sources, treat these as conceptual ranges and planning templates, not medical prescriptions.
Pattern A: “Sustained BPC-157 + Shorter TB-500 Cycle” (widely discussed)
This approach is typically chosen to keep BPC-157 steady for a longer recovery window while using TB-500 for a shorter cycle.
- BPC-157: often planned as a daily or near-daily dosing schedule for multiple weeks.
- TB-500: often planned as a shorter series (commonly discussed as starting early in the stack), then reassessed.
Why this pattern is popular: It aims to provide consistent support while preventing the protocol from becoming too “heavy” for the entire duration.
Pattern B: “Early TB-500 + Longer BPC-157” (flare/return-to-training focus)
Some people time TB-500 earlier when they’re trying to calm issues and improve function so they can start progressive training again, while BPC-157 remains the longer support.
- TB-500: placed earlier to match the period when activity limitation is greatest.
- BPC-157: used across the later phase when you’re trying to maintain gains and reduce setbacks.
In my hands-on view: This can make sense when your injury or overuse flare tends to respond slowly, and you want to focus support where it’s most limiting.
Pattern C: “Both on the same timeline” (simple adherence)
If you’re prone to schedule drift, pairing both on the same overall timeline can be easier to follow.
- BPC-157 and TB-500: dosed on a consistent schedule for a defined stack period.
Tradeoff: Simpler schedule, but you may not be targeting the “most limiting” phase as effectively as Pattern A or B.
Injection Practicalities: How I Plan a Stack to Reduce Mistakes
Even a good idea fails if the execution is sloppy. Here’s how I structure peptide protocols to minimize avoidable errors.
1) Use a written schedule and single source of truth
I keep a one-page plan that lists day-by-day doses, injection times, and how I’ll measure outcomes. If your plan lives only in your head, you’ll eventually miss a dose or change timing—then you’ll struggle to interpret whether something helped.
2) Track objective recovery markers, not just “feeling better”
For musculoskeletal recovery, I typically include:
- Pain score at rest and during the specific movement
- Range of motion limits (before/after activity)
- Swelling or localized tenderness (simple scale)
- Training readiness (e.g., whether you can return to the same load)
3) Plan your activity load around the stack window
Peptides don’t replace good biomechanics and progressive loading. When we’ve seen the most improvement, the people involved used the stack window to gradually increase activity while reducing irritators—rather than trying to “push through” pain.
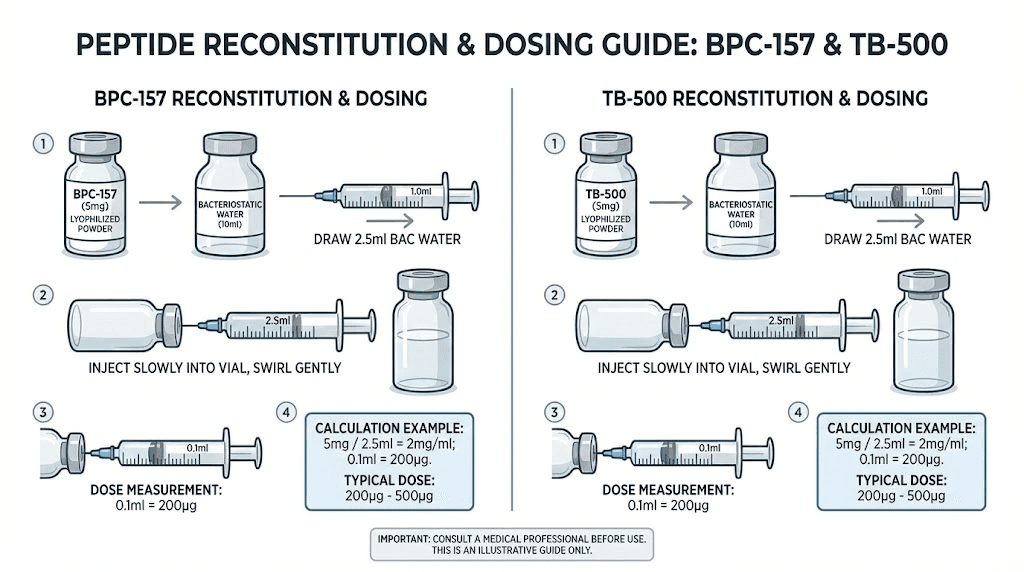
Product Image
Safety, Limitations, and What to Watch For
Peptide stacking is often discussed online with confidence, but the reality is that individual responses vary and non-clinical protocols carry risks. Here’s what I emphasize in practice.
Possible limitations
- Variable product quality: Different suppliers and batches can differ.
- Confounded results: Training changes, sleep, and anti-inflammatory habits can mimic “stack” effects.
- Not all pain is the same: Tendon, ligament, muscle strain, and joint irritation respond differently to recovery strategies.
When to pause and get medical advice
- New or worsening pain patterns
- Significant swelling, heat, or redness
- Unusual symptoms after starting a protocol
- If you’re on medications or have conditions where peptide use could be higher risk
Bottom line: If your goal is accelerated healing, you still need a conservative, monitoring-first approach. I’ve seen protocols fail because people treated dosing like the only variable.
How to Choose Your First Stacking Plan (A Practical Workflow)
Use this sequence to design a stack that you can actually follow and evaluate.
- Define the target: What are you recovering from (strain, overuse, post-activity irritation)?
- Set baseline metrics: Record pain and function for 3–5 days before starting.
- Pick a stacking pattern: Choose Pattern A, B, or C based on how hard your schedule will be to maintain.
- Decide your bpc 157 and tb500 dosage structure: Keep dosing timing consistent and document it.
- Control training variables: Keep irritants stable; progress load only if your markers improve.
- Review after a defined window: Decide in advance what “enough evidence” looks like (e.g., improved range of motion or reduced pain during a specific movement).
FAQ
What’s the best bpc 157 and tb500 dosage stack for accelerated healing?
There isn’t one best universal dosage. The best approach is the one you can follow consistently while tracking outcomes, using a stacking pattern that matches your recovery timeline (for example, sustained BPC-157 with a shorter TB-500 cycle). Any numeric choices should be guided by clinician advice and product-specific labeling/potency.
How long should a BPC-157 and TB-500 stacking cycle last?
People commonly plan multi-week windows for BPC-157 and shorter TB-500 cycles, but exact duration depends on injury type, baseline severity, and training/activity load. The practical rule is to set a predefined evaluation window and base continuation on objective improvements, not expectations.
Can I adjust dosage if I don’t feel improvement quickly?
Rather than jumping dose quickly, I recommend first checking adherence (timing missed?), confounders (sleep, load, irritators), and whether your pain source matches the protocol’s typical target. If you’re not seeing improvement after your planned checkpoint, reassess with a qualified clinician rather than repeatedly changing variables.
Conclusion
Stacking BPC-157 and TB-500 for accelerated healing is less about finding a “magic” formula and more about building a coherent, trackable plan. In my hands-on experience, the strongest outcomes come from consistent scheduling, baseline tracking, and smart training load management—while keeping safety and product variability in mind.
Next step: Create a one-page protocol for your first stack cycle with (1) your chosen stacking pattern, (2) your bpc 157 and tb500 dosage schedule structure, and (3) 3–4 objective recovery markers you’ll measure before and during the trial.
Discussion