How To Give A B12 Injection In The Deltoid Deltoid Intramuscular injection - Everything You Need To Know
Introduction
If you’ve ever been handed a medication order and thought, “I can do it with confidence… but how do I actually give the injection safely in the first place?”, you’re not alone. The deltoid intramuscular route is common for certain injections, but the margin for error is real—wrong site selection, poor needle technique, or an injection done at the wrong depth can make the experience needlessly painful or complicate healing.
In this guide, I’ll walk you through deltoid intramuscular injection basics with a practical focus on how to give a b12 injection in the deltoid—including site selection, needle angle, depth, technique, and what to watch for afterward.
What a Deltoid Intramuscular Injection Is (and Why Site Selection Matters)
An intramuscular (IM) injection delivers medication into the muscle tissue to help with absorption. The deltoid is one of the most accessible IM sites, especially for small-volume injections and self-administration when appropriate.
In my hands-on work training patients and caregivers, the biggest recurring problems weren’t “needle fear”—they were:
- Choosing the wrong location on the upper arm (too high toward the shoulder joint or too far toward the back of the arm).
- Incorrect needle angle and inconsistent depth, leading to medication going into subcutaneous tissue instead of muscle.
- Rushing the prep steps (not cleaning long enough, reusing equipment, or not letting the skin fully dry).
The logic is simple: IM absorption relies on consistent placement in the targeted muscle. If placement is off, you may see more soreness, swelling, or unpredictable absorption.
How to Give a B12 Injection in the Deltoid: Step-by-Step Technique
This section focuses on the common practical scenario: how to give a b12 injection in the deltoid. Always follow your prescriber’s instructions and the medication’s label (including volume, needle gauge/length, and any special guidance).
1) Gather what you need (and keep it clean)
- Medication (B12) and the correct syringe
- Needle per your instructions
- Alcohol swabs or appropriate skin disinfectant
- Sharps container (or a puncture-resistant disposal option)
- Clean gauze/cotton for light pressure if needed
My practical rule: If anything isn’t laid out before you start, you’re more likely to touch non-sterile surfaces mid-procedure.
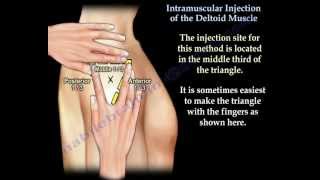
2) Choose the correct injection site on the deltoid
The deltoid site is typically the “middle” of the upper outer arm. A reliable method is to locate the bony landmarks and place the injection in the muscle belly that sits slightly below the shoulder contour and above the upper arm curvature.
Key guidance I teach:
- Use the upper outer arm (lateral part).
- Avoid injecting too high near the shoulder joint.
- Avoid injecting too far back or toward the inner arm.
3) Prep your skin
- Wash your hands thoroughly.
- Use an alcohol swab to clean the deltoid area.
- Let the skin dry fully before injecting.
Letting the skin dry matters. In training sessions, I’ve seen people inject while the area is still wet, which can increase surface irritation and sting.
4) Position the arm
Seat the person comfortably. The arm should be relaxed, with minimal tension. If the deltoid is tense, the injection often feels sharper and recovery can feel slower.
5) Insert the needle at the right angle
For deltoid IM injections, the needle is generally inserted at an angle appropriate to the needle length and technique your clinician prescribed.
In real-world practice: Many clinicians teach a straightforward approach—insert confidently into the muscle, using the prescribed needle length—rather than stopping halfway “to be safe.” Stopping too early is a common cause of medication landing in subcutaneous tissue.
6) Inject the medication slowly and consistently
Injecting steadily (rather than jabbing the plunger fast) can reduce discomfort. Once finished, keep gentle pressure and avoid sudden movements.
7) Remove the needle and manage the site
- Withdraw the needle straight out.
- Apply light pressure with gauze/cotton if needed.
- Do not rub vigorously.
- Dispose immediately into a sharps container.
8) What you should expect afterward
- Common: mild soreness, slight redness, or a small tender area.
- Less common: bruising, a firm lump that improves over time, or increased soreness lasting a bit longer.
- Not normal: rapidly worsening swelling, severe pain, warmth spreading outward, or signs of infection.
In follow-ups, I’ve found most discomfort improves with time and good aftercare—cool compress for the first day if advised, and gentle mobility to avoid stiffness.
Needle, Depth, and Volume: Getting the “Fit” Right
Deltoid injections are best suited when the prescribed needle and medication volume match the deltoid route. If the volume is too large for the deltoid, pain and tissue irritation can increase. If the needle is too short for the person’s anatomy, you risk placing the medication too superficially.
Practical considerations I look for
- Needle length and gauge as instructed by the prescriber/pharmacy.
- Body habitus: muscle thickness can vary, affecting depth needs.
- Medication characteristics: some formulations are more viscous, which can change how smoothly they inject.
Bottom line: Technique matters, but the “fit” between needle choice, injection site, and medication volume is equally important.
Step Quality: Common Mistakes (and How to Avoid Them)
Here are the issues I most often see when people are learning, and what to do instead:
- Missed landmarking: People inject too close to the shoulder joint. Fix by clearly identifying the deltoid muscle belly (outer, mid-portion of the upper arm).
- Not disinfecting properly: Quick wipes that don’t allow drying can sting and irritate. Fix by swabbing and letting it dry.
- Inconsistent depth: Stopping too early can reduce IM placement accuracy. Fix by inserting to the intended depth per training and needle length.
- Rushing disposal: Leaving used needles exposed is a preventable hazard. Fix by having the sharps container ready before starting.
Illustration: Deltoid IM Injection Site
Aftercare and Safety: When to Seek Help
Most people experience mild soreness and minor redness. However, safety is non-negotiable. Get medical advice promptly if there’s:
- Severe or escalating pain
- Large swelling, spreading redness, or increasing warmth
- Fever or pus
- Signs of an allergic reaction (e.g., hives, facial swelling, trouble breathing)
- Persistent symptoms that don’t improve over time
If you’re unsure whether you placed the injection correctly, or you feel resistance was unusual, it’s reasonable to contact your clinician for guidance on next steps.
FAQ
Can I self-administer a B12 injection in the deltoid?
Many people can—if the prescription, needle plan, and your ability to identify the correct deltoid site are appropriate. If you’re uncertain about landmarks or needle technique, ask your clinician or pharmacist for hands-on instruction before attempting it independently.
How long should soreness last after a deltoid B12 injection?
Mild soreness and tenderness often improve within a day or two. If pain is worsening, the area is hot or increasingly swollen, or symptoms persist beyond what your clinician considers normal for that medication, seek medical advice.
What’s the most important thing to get right for how to give a b12 injection in the deltoid?
The most critical factors are correct site selection (upper outer deltoid muscle belly) and placing the needle at the intended depth using the prescribed needle and technique.
Conclusion
A deltoid intramuscular injection is a straightforward procedure only when the fundamentals are consistent: correct landmarking, proper skin prep, correct needle technique, and appropriate aftercare. For how to give a b12 injection in the deltoid, the goal is reliable muscle placement to support predictable absorption and a smoother recovery.
Next step: Before your next dose, do a dry-run visualization—identify the deltoid site on your arm, then review the needle plan and injection steps with your clinician or pharmacist so the real-time technique matches what you practiced.
Discussion