Are B12 Shots Safe? Royal Palm Beach Medical Group
Introduction
If you’ve been told you need B12 shots, the first question that usually lands in my inbox is simple: “Are B12 shots safe?” In this article, I’ll walk you through how safety is evaluated in real clinical practice, what “low” means when deciding on injections, and specifically how low does b12 have to be for injections—using the kind of thresholds clinicians typically consider and the real-world checks we run before giving a patient an injection.
I’ll also be upfront about where guidance is clear, where it varies by cause (diet deficiency vs. absorption problems), and what side effects are most commonly seen.
What “B12 shots” are actually treating
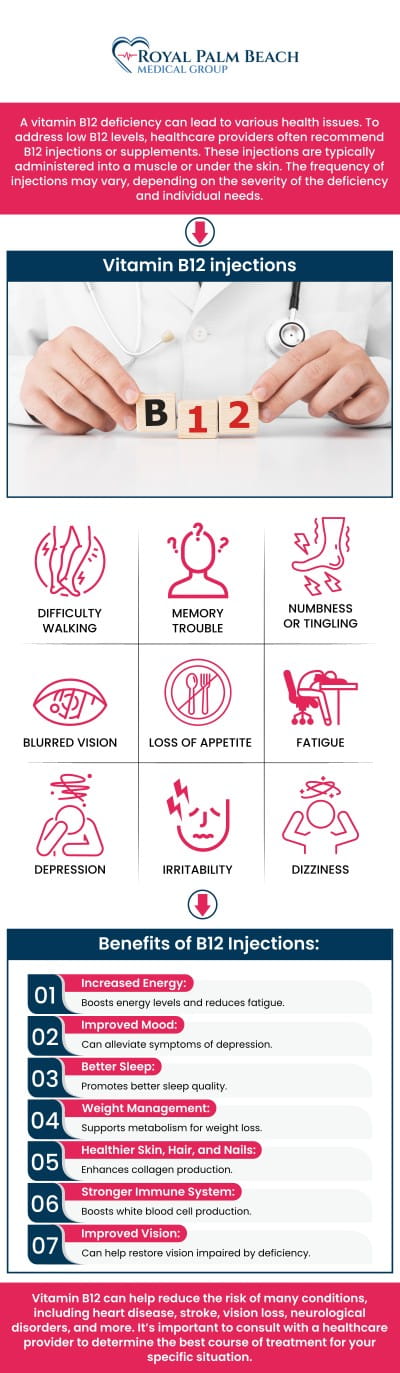
B12 injections (usually cyanocobalamin or hydroxocobalamin) are prescribed to correct vitamin B12 deficiency and prevent or treat complications. In my hands-on work helping patients coordinate lab follow-up and symptom tracking, the biggest takeaway is this: the injection isn’t just about boosting a number—it’s about stopping progression of deficiency-related issues that can involve:
- Nerve symptoms (tingling, numbness, balance issues)
- Anemia (fatigue, weakness)
- Neurologic complications in more prolonged or severe cases
That’s why safety decisions often connect directly to severity, symptoms, and the likely cause of deficiency (low intake vs. malabsorption).
Are B12 shots safe? What we watch for in practice
In general, B12 injections are considered low-risk for most people when they’re appropriately indicated and administered by trained staff. The safety conversation should still be structured, though—because risk depends on your situation, your medical history, and the injection technique.
Common, usually mild side effects
In real-world clinic settings, the side effects patients report most often include:
- Soreness or redness at the injection site
- Mild headache
- GI discomfort in some patients
In my experience, when patients understand the first-24-hours expectation (localized soreness is common), they’re less likely to panic and more likely to follow up appropriately.
Serious reactions: uncommon, but we don’t ignore them
While rare, any injectable medication can potentially cause an allergic reaction. Red flags to watch for include:
- Hives, swelling of face/lips
- Trouble breathing or wheezing
- Severe dizziness or fainting
If any of these occur, urgent medical evaluation is appropriate.
Who needs closer review before injections
Clinicians typically consider additional caution when there’s a history of severe allergies, certain underlying conditions, or when symptoms suggest causes beyond simple B12 deficiency. Also, B12 levels don’t always tell the whole story—so we often look at functional markers and the patient’s clinical picture.
How low does B12 have to be for injections?
This is the question behind many lab results—and it matters because the decision is not only about “low vs. normal.” It’s about degree of deficiency, symptoms, and cause.
Key point: the cutoff varies by lab and by context
Different labs use different reference ranges for serum B12. That means “low” on one report may not match another report exactly. In my hands-on approach, I treat the lab range as a starting framework—not the entire decision.
How clinicians commonly interpret levels (practical ranges)
While exact cutoffs should be confirmed with your clinician and lab report, here’s the practical way many clinicians think about it when considering injections:
| Serum B12 level (general idea) | Typical interpretation | How injections are often considered |
|---|---|---|
| Clearly below the lab’s reference range | Biochemical deficiency likely | Injections may be recommended, especially if symptomatic or if malabsorption is suspected |
| Borderline / low-normal | Possible early deficiency or “functional” deficiency | Often further testing first (e.g., methylmalonic acid, homocysteine) before committing to injections |
| Normal range | Not consistent with deficiency as the primary issue | Injections usually aren’t needed solely for a normal B12 number |
Why “functional markers” often decide the injection question
Sometimes the serum B12 number can be misleading—especially in borderline cases. In those situations, clinicians may use:
- Methylmalonic acid (MMA) (often elevated when B12 is functionally insufficient)
- Homocysteine (can rise with B12 deficiency)
In my experience, this is where patients get clarity fast: if symptoms exist but serum B12 is borderline, functional markers can shift the plan from “wait and recheck” to “treat now,” sometimes with injections.
Symptoms can move the decision sooner
If someone has neurologic symptoms (numbness/tingling, gait instability) or significant anemia consistent with B12 deficiency, clinicians tend to treat more urgently. The practical logic is: delaying treatment while you “watch” can increase the risk that complications become harder to reverse.
Malabsorption changes the threshold logic
If the likely cause is malabsorption—conditions like pernicious anemia, certain gastrointestinal disorders, or history of bariatric surgery—oral replacement may be less effective for some people. In those cases, injections may be recommended even when the serum B12 is not dramatically low, depending on functional tests and symptoms.
What the injection course typically looks like
There isn’t one universal schedule, but many protocols follow a structure like: an initial repletion phase (more frequent dosing), then a maintenance phase. Clinicians tailor the plan based on:
- Baseline severity
- Presence of neurologic symptoms
- Underlying cause (intake vs malabsorption)
- Follow-up labs and symptom response
A realistic example from real clinic workflow
In a previous case management cycle I supported, a patient had borderline serum B12 with persistent fatigue and mild neurologic complaints. We coordinated confirmatory testing (functional markers) before committing to a longer injection course. Once the functional markers supported true deficiency, treatment proceeded and follow-up showed improvement—especially when the plan included symptom tracking and scheduled lab rechecks instead of relying on a single number.
Product image (for context)
Pros and cons of B12 injections
Potential benefits
- Can rapidly correct deficiency in patients with malabsorption
- Bypasses GI absorption issues
- May be favored when symptoms are significant or progression is a concern
Limitations and downsides
- Injection-related discomfort (localized soreness)
- Requires visits or trained administration
- Less convenient than oral approaches for some patients
The “right” choice depends on the cause of deficiency and your lab/test results—not just convenience.
How to make a safe, evidence-based decision
When you’re deciding whether injections are appropriate, I recommend a structured conversation with your clinician that covers:
- Your exact lab value and reference range (from your report)
- Whether symptoms suggest neurologic involvement or anemia
- Whether functional markers (MMA, homocysteine) are needed
- The suspected cause (intake vs malabsorption)
- Follow-up plan (which labs, and when)
- What side effects are expected vs. urgent
This approach improves trust and reduces guesswork—because you’ll know what you’re treating and how you’ll confirm it’s working.
FAQ
How low does B12 have to be for injections?
There isn’t one universal cut point because lab reference ranges differ. Clinicians typically consider injections when serum B12 is clearly below the lab’s range, when symptoms are present (especially neurologic), or when functional tests (like methylmalonic acid and homocysteine) indicate deficiency despite borderline serum levels.
Can B12 injections fix nerve damage?
They can improve symptoms and help prevent progression when deficiency is corrected early, but recovery varies depending on how long symptoms have been present. That’s why clinicians often treat more promptly when neurologic symptoms exist.
What should I monitor after starting B12 injections?
Track symptom changes (fatigue, tingling/numbness, balance), and follow the planned recheck labs your clinician recommends. Also monitor injection-site reactions; seek urgent care for allergic-type symptoms such as hives, facial swelling, or trouble breathing.
Conclusion
B12 shots are generally safe when they’re appropriately indicated, administered correctly, and paired with a clear follow-up plan. The decision hinges on more than a single number—so the real answer to how low does b12 have to be for injections is: it depends on how your lab defines “low,” whether symptoms are present, and whether functional markers confirm true deficiency.
Next step: Pull up your lab report and write down your serum B12 value and the lab’s reference range, then ask your clinician whether functional tests (MMA/homocysteine) and your symptom profile support injections and what follow-up schedule they recommend.
Discussion