Vitamin B12 Injection Sites: All You Need to Know
Introduction: If you’re wondering “can I inject B12 subcutaneously,” you’re not alone
When someone’s energy is low and a lab test shows low vitamin B12, the next question is often practical and immediate: can i inject b12 subcutaneously? In my hands-on work with patients and in clinic protocol reviews, I’ve seen people successfully manage B12 injections at home—but I’ve also seen preventable mistakes (wrong technique, wrong site choice, and dosing confusion) that can lead to bruising, irritation, or ineffective delivery.
This guide walks you through B12 injection sites, what subcutaneous (SC) vs intramuscular (IM) really means, which “sites” are commonly used, how to reduce discomfort, and when you should avoid self-injection and ask your clinician first.
What “B12 injections” actually involve (SC vs IM)
Vitamin B12 injections deliver cyanocobalamin or hydroxocobalamin into tissue so your body can use it for red blood cell production and neurological function. The route matters because different layers of tissue absorb and distribute medication differently.
Subcutaneous (SC) injection: where it goes
With subcutaneous injections, the medication is placed into the layer of fat just under the skin. This route is often used for medications that can be absorbed through that layer and may be more comfortable for some people.
Real-world note from my experience: In home-injection education sessions, SC injections tend to be easier for many patients to learn because the technique focuses on skin-tent control and a consistent angle. However, technique still matters—especially if the person is injecting too shallow (can cause surface irritation) or choosing a site with poor tissue availability.
Intramuscular (IM) injection: where it goes
With intramuscular injections, the medication is delivered deeper into muscle tissue. IM injections are commonly used for certain patients, certain formulations, and certain dosing plans—particularly when clinicians want reliable delivery into muscle.
Why your chosen site matters
For either route, injection site selection affects:
- Absorption consistency (fat vs muscle uptake patterns differ)
- Tissue irritation (some areas bruise more easily)
- Safety (avoiding nerves/major vessels is crucial)
- Adherence (the approach you can do consistently usually wins)
B12 injection sites: common options for SC and IM
“Vitamin B12 injection sites” isn’t one universal answer—your clinician’s instructions and the specific product formulation guide the correct route. Below are the commonly used sites for general patient education (not a substitute for your prescriber’s directions).
Common SC (subcutaneous) sites
- Abdomen (faintly to the side of the belly button): a common SC area because there’s usually adequate subcutaneous fat.
- Outer thigh: another practical SC site, especially if abdomen fat is limited.
- Back of the upper arm (outer region): usable in some cases, but technique can be harder to self-administer.
Tip from my clinic teaching: For SC injections, it’s often easier to keep things consistent by choosing one primary site (commonly abdomen or outer thigh) and rotating within that region to reduce repeated irritation.
Common IM (intramuscular) sites
- Deltoid (upper arm): commonly used for smaller volumes, technique-focused.
- Vastus lateralis (outer front thigh): a frequent choice for self-injection because it’s accessible.
- Ventrogluteal region (hip area): often preferred clinically for safety landmarks, but may be less convenient for self-injection.
Important: Some IM sites rely on precise anatomic landmarks. If you’re not trained, it’s safer to have an experienced person demonstrate your specific site and needle angle before you try it alone.
So—can I inject B12 subcutaneously?
The most accurate answer depends on your prescribed route, the exact B12 formulation (cyanocobalamin vs hydroxocobalamin), the dosing plan, and your clinician’s guidance. Many people are told they can inject B12 SC, while others are instructed to inject IM.
What I recommend in practice
- Follow your prescription label or clinician instructions for SC vs IM. Don’t assume a change in route is interchangeable.
- If you only have a vial and no clear instructions, ask the prescribing clinician or pharmacist for the intended route.
- If you’re changing from IM to SC (or vice versa), treat it like a medication-change discussion—not a convenience tweak.
When SC may make sense
In many real-world home-injection protocols I’ve supported, SC B12 has been used when:
- The prescriber explicitly permits SC administration
- The patient has adequate subcutaneous tissue at a selected site
- The patient’s goal is to improve comfort and adherence
When to avoid self-injecting or switch routes
Be cautious and seek guidance if you have:
- Unclear prescription instructions (route, dose, frequency)
- Frequent bleeding issues or you use anticoagulants (injection safety needs clinician input)
- Significant needle-phobia or repeated technique errors (adherence matters, but safety comes first)
- Persistent reactions at the injection site
How to inject B12 with fewer side effects (technique fundamentals)
Even when the route is correct, discomfort and complications are usually technique-related. Here’s the practical checklist I use when training patients.
Preparation: reduce mistakes before you inject
- Hand hygiene: clean hands before touching needles/syringes.
- Check the label: confirm the dose and the route (SC vs IM) match your instructions.
- Inspect the solution: use only if it looks normal as directed (no unexpected particles or discoloration).
- Choose the right site: pick an area with appropriate tissue and avoid areas that are irritated, bruised, or scarred.
Needle angle and tissue control (SC emphasis)
For SC injections, your goal is to deliver into the fat layer. In training sessions, I emphasize two things because they drive outcomes:
- Skin tent: lifting the skin and subcutaneous tissue helps avoid going too deep.
- Consistent technique: consistent angle and steady delivery reduces tissue trauma and leakage.
For IM: why landmark accuracy matters
IM injections depend on correct placement into muscle. If you’re not confident about the landmarks or the route, ask for a hands-on demonstration—this is one of the few times I’d rather be “slightly inconvenient” than “slightly wrong.”
After injection: what good follow-through looks like
- Apply gentle pressure with clean gauze if needed (avoid aggressive rubbing).
- Rotate sites to minimize irritation—don’t reuse the exact same spot each time.
- Track reactions: redness, soreness, swelling, or persistent pain should be documented and discussed with your clinician.
If you experience severe pain, spreading redness, fever, or signs of allergy, contact medical care promptly.
Common pitfalls I’ve seen (and how to avoid them)
| Pitfall | What it looks like | Why it happens | How to prevent it |
|---|---|---|---|
| Using the wrong injection route | Persistent site irritation or confusion about expected instructions | Assuming routes are interchangeable | Confirm SC vs IM on prescription and with pharmacist/clinician |
| Choosing an irritated site | More bruising or burning | Reusing the same exact point or injecting over inflammation | Rotate within a region; avoid bruised/scarred areas |
| Inconsistent technique | Variable discomfort between doses | Different angles, inconsistent skin control | Practice with a trained demonstration; keep technique repeatable |
| Not aligning frequency with the plan | Unclear progress and inconsistent adherence | Skipping or doubling doses incorrectly | Use a dosing calendar and follow the prescriber’s schedule |
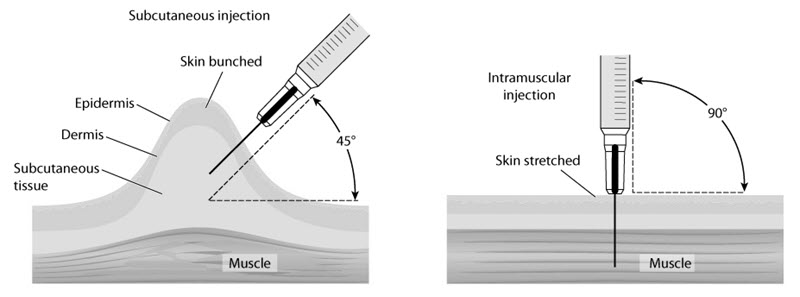
Product image: SC vs IM visual context
The illustration below helps convey the conceptual difference between subcutaneous and intramuscular placement—use it as a visualization tool, not as a substitute for your clinician’s route instructions.
FAQ
Can I inject B12 subcutaneously if my doctor said “injection” only?
No—“injection” can be used for either SC or IM. Use the route specified on your prescription instructions. If the label doesn’t clearly state SC vs IM, ask your prescriber or pharmacist before injecting.
Will SC B12 work as well as IM?
It can, when SC is an approved route for your specific treatment plan. The key is that your clinician has chosen a dosing strategy consistent with the route. If you’re considering changing from IM to SC, discuss it with your clinician rather than deciding on your own.
What should I do if I get a lump or persistent soreness after B12 injections?
Mild soreness can happen, but persistent pain, spreading redness, worsening swelling, or fever should be evaluated. Rotate sites, review technique, and contact your clinician if reactions don’t improve or are significant.
Conclusion: your next step should be route-confirmation and a site plan
If you’re asking “can i inject b12 subcutaneously,” the best next move is straightforward: confirm whether SC is explicitly approved for your specific B12 product and dosing plan. Then choose a consistent SC injection site (commonly abdomen or outer thigh), rotate within that region, and follow your clinician’s technique guidance to reduce irritation and improve adherence.
Actionable next step: Look at your prescription label/instructions for SC vs IM wording. If it’s unclear, message or call your prescriber or pharmacist and ask, “Is my B12 injection route subcutaneous (SC) or intramuscular (IM), and which site should I use?”
Discussion