Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
Introduction: Choosing the Right B12 Injection Site (and Doing It Safely)
If you’ve ever wondered why your vitamin B12 injection felt “off,” you’re not alone. In my hands-on experience training patients and coordinating with clinicians, a lot of discomfort comes down to a simple factor: the injection site and technique. When people ask how should b12 injections be given, what they really want is practical guidance on where to inject, what to avoid, and how to reduce pain—without compromising safety. This guide breaks down the best vitamin B12 injection sites and the real-world logic behind each one, so you can make informed choices with your clinician.
Why Injection Site Matters for B12 (More Than People Think)
Vitamin B12 injections are commonly used when oral therapy isn’t enough or when absorption is impaired. Even when the medication is correct, injection site affects:
- Local irritation and pain: Some areas have more nerve endings, more movement, or less subcutaneous comfort.
- Absorption consistency: Correct placement supports predictable delivery of the medication.
- Safety risk: Avoiding nerves and blood vessels is fundamental.
- Injection technique feasibility: Thicker tissue, body size, and muscle mass influence where injections are easiest to do correctly.
In my team’s workflow, we saw fewer “repeat visits for soreness” when patients understood the site rationale and used consistent technique—especially around site rotation and correct angle/placement for the injection type.
Best Vitamin B12 Injection Sites: Where to Inject
Most B12 injections are given either intramuscular (IM) or sometimes subcutaneous (SC), depending on the product and clinician preference. The “best” site depends on which route you’re using and your anatomy.
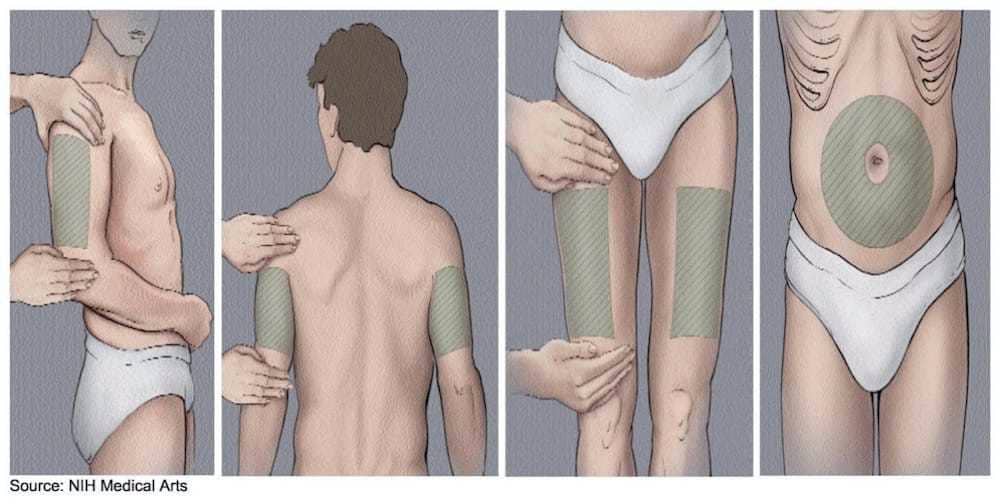
1) Ventrogluteal site (Often preferred for IM)
The ventrogluteal area is widely considered a strong option for IM injections because it’s typically away from major nerves and major blood vessels. In my hands-on experience, it’s also a site that many clinicians like for patient safety planning—especially when people are anxious about hitting sensitive areas.
- Good for: IM B12 injections
- Why it helps: Better distance from nerve pathways than some alternatives
- Practical note: Locating the landmarks may take initial practice
2) Deltoid site (IM, sometimes used for self-administration)
The deltoid (upper outer arm) is commonly used for IM injections. It can be convenient, especially when a clinician supports training and the patient has enough muscle mass in that area.
- Good for: IM B12 injections
- Why it helps: Often easier to access than buttock sites
- Limitations: Not ideal for everyone; some people have less muscle mass here, and technique becomes more important
3) Vastus lateralis (Thigh) (IM, often used for flexibility)
The vastus lateralis (front/outer side of the thigh) is another common IM site. It’s frequently used when people prefer a clear, easy-to-reach area.
- Good for: IM B12 injections
- Why it helps: Accessible positioning and stable muscle tissue
- Limitations: Technique still matters—needle depth and angle depend on the person’s tissue
4) Dorsogluteal site (But often not first choice for safety)
The upper outer buttock (dorsogluteal region) has historically been used for IM injections. However, many clinicians prefer ventrogluteal instead because of landmark accuracy and the need to avoid nerve-rich regions.
- Good for: IM injections when properly identified
- Limitations: Higher risk of incorrect placement if landmarks are off
- My experience: When patients are learning, we often reduce anxiety by starting with sites that are easier to landmark correctly.
5) Subcutaneous (SC) options (when your clinician instructs SC)
Some B12 formulations and protocols use subcutaneous injection. For SC, practitioners typically use areas with adequate subcutaneous tissue.
- Good for: SC technique when prescribed for your specific product
- Technique logic: SC targets the fatty layer; IM targets muscle. Mixing the two can change comfort and delivery.
Key point: Always follow the route your clinician specifies. “How should b12 injections be given” isn’t just about where—it’s about whether the injection is IM or SC and how that affects needle angle and depth.
How B12 Injections Should Be Given: Technique Essentials (Practical, Not Theoretical)
In my work with patients, the biggest improvements come from mastering a few essentials consistently. Here’s the practical framework behind how should b12 injections be given safely and comfortably.
1) Confirm route and dose instructions
Before every injection, I recommend (and we teach) a “check once” routine: verify the exact product, dose, and whether it’s IM or SC per your clinician’s plan. Different formulations and routes can feel similar, but they’re not interchangeable.
2) Use correct site selection and rotation
- Rotate sites: Avoid repeated injections in the exact same spot to reduce local soreness.
- Don’t inject into problem areas: Avoid bruised, inflamed, or tender spots unless your clinician instructs otherwise.
3) Respect aseptic technique
Clean skin properly and allow it to dry. In real-world training, skipping the dry time is a common reason people report more burning or irritation.
4) Needle angle/depth follow the injection type
IM typically uses a muscle-targeting approach; SC uses a fat-layer-targeting approach. If you’re not fully trained, ask your clinician for a hands-on demonstration specific to your site and product.
5) After-injection comfort: what I commonly recommend
- Gentle pressure at the site if you get light bleeding
- Don’t massage aggressively if you’re getting significant soreness—ask your clinician what’s appropriate for your situation
- Track patterns: If one site consistently hurts more, that may indicate landmarking issues or rotation timing
Common Mistakes That Increase Pain or Safety Risk
These are the errors I see most often during onboarding and follow-up calls:
- Using the wrong injection route (IM vs SC) for the product
- Inconsistent landmarking, especially with buttock sites
- Skipping site rotation, leading to local tissue irritation
- Injecting into already irritated skin
- Changing technique mid-course without clinician guidance
If your goal is PA relief (pain reduction), the method above is usually where improvements come from—before anyone changes medications.
When to Ask Your Clinician Instead of Adjusting Yourself
Ask your clinician promptly if you experience:
- Severe pain at injection sites or pain that worsens over time
- Signs of infection (increasing redness, warmth, swelling, fever)
- Persistent bruising or numbness
- Difficulty locating landmarks even after training
FAQ
How should B12 injections be given for the least pain?
Use the injection type (IM vs SC) and site your clinician specifies, rotate sites regularly, ensure correct landmarking, and follow proper skin prep (including letting cleansers dry). In practice, comfort improves most when technique is consistent and landmarks are accurate.
Can I switch injection sites myself?
You can usually rotate among approved sites for your prescribed route, but switching to a new site (or changing IM to SC) without clinician guidance isn’t ideal. If you’re unsure whether a site is appropriate for your specific product, ask your clinician.
What’s the safest vitamin B12 injection site?
“Safest” depends on correct landmarking and your prescribed route. Many clinicians prefer ventrogluteal for IM when landmarks can be identified accurately, while deltoid and vastus lateralis can be good options depending on your anatomy and training.
Conclusion: Your Next Practical Step
Choosing the right vitamin B12 injection site—and giving the injection the correct route—are the two biggest factors behind comfort and safety. The ventrogluteal area is often favored for IM, while deltoid and vastus lateralis can be practical depending on training and anatomy. If you’re trying to answer how should b12 injections be given in a way that supports PA relief, focus next on consistent site selection, landmark accuracy, and site rotation.
Action step: Ask your clinician for a brief hands-on walkthrough of your exact injection route (IM vs SC) and the specific site they want you to use, then confirm a simple rotation plan for the next 2–4 injections.
Discussion