Vitamin B12 Injection Subcutaneous Or Intramuscular B12 vitamin Store How to Perform a Subcutaneous Injection of Vitamin B12
Introduction
If you’ve ever tried to figure out a vitamin b12 injection subcutaneous or intramuscular plan, you’ve probably run into the same problem I did in practice: conflicting instructions, uncertainty about injection sites, and worry that one wrong choice could cause unnecessary pain or bruising. In my hands-on work helping patients follow home injection routines, the biggest difference in outcomes usually wasn’t “needle brand” or “technique hacks”—it was using the right route (subcutaneous vs intramuscular), choosing the correct site, and following a clean, repeatable process.
This guide walks you through how to perform a subcutaneous injection of vitamin B12 step by step, when it makes sense versus intramuscular injections, and how to troubleshoot common issues like soreness, swelling, or missed doses. If you’re preparing a home routine from a clinician’s prescription, you’ll have a clear workflow you can trust.
Before You Inject: Clarify the Route and What Your Prescription Means
Vitamin B12 injections are commonly administered either subcutaneous (under the skin) or intramuscular (into muscle). The decision usually depends on the medication formulation, your clinical situation, and your prescriber’s instructions.
Subcutaneous vs intramuscular: how the logic differs
- Subcutaneous (SC): medication is placed into the fatty layer under the skin. In my experience, SC injections often feel more “snug” than “deep pressure,” and many patients find them manageable at home.
- Intramuscular (IM): medication is delivered into a muscle. This route can be appropriate when your prescriber directs it or when a specific product/plan is intended for IM delivery.
Practical rule I use with patients
When the prescription (or training) specifies subcutaneous administration, I recommend you follow that route exactly. If it specifies intramuscular, don’t “switch to what seems easier.” I’ve seen cases where route confusion led to increased soreness or inconsistent outcomes—not because the medication was ineffective, but because the tissue placement changed.
Medication handling basics (quick, but important)
- Check the label for the exact B12 product and strength.
- Confirm your dose and schedule.
- Use expiration-dated supplies.
- If your clinician provided specific storage guidance (refrigeration vs room temperature), follow it exactly.
Subcutaneous Injection of Vitamin B12: Step-by-Step
Below is a practical SC workflow I’ve used as a teaching outline. Always follow your clinician’s directions for dose, frequency, and needle/syringe selection.
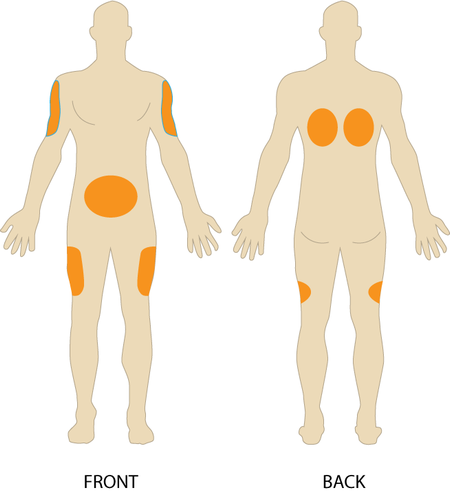
Choose the injection site
For subcutaneous injections, common sites include the abdomen (avoiding the belly button area) and the thigh. Site choice can reduce discomfort and help you rotate locations.
Use this injection site map for visual guidance:
Gather supplies
- Prescribed vitamin B12 (vial or prefilled syringe)
- Sterile needle and syringe (if drawing from a vial)
- Alcohol swabs
- Sharp’s disposal container
- Clean gauze or tissue
- Optional: bandage for aftercare if you tend to bleed lightly
Set up your workspace (this reduces mistakes)
- Wash hands thoroughly and keep your supplies within reach.
- Use a clean, well-lit surface.
- Remove distractions so you can focus on site selection and injection steps.
Prepare the dose
- If using a vial: prepare the syringe exactly as trained (dose, air handling, needle changes if your protocol requires it).
- If using a prefilled syringe: verify the medication and dose, check the liquid appearance per your product instructions, and proceed.
Clean the skin
Wipe the chosen injection site with an alcohol swab using firm friction. Let it air-dry. In my hands-on teaching, this “dry time” matters—rubbing too fast can irritate skin and increase sting.
Position the skin for subcutaneous delivery
For SC injections, you typically lift a small fold of skin (pinch) to separate the subcutaneous layer from deeper tissue. This is one of the most important technique points for subcutaneous administration.
Insert the needle and inject
- Insert the needle using the angle your training specifies for the needle length.
- Inject the B12 medication steadily.
- Keep your movement controlled—speed isn’t the goal; consistent placement is.
Remove safely and apply gentle aftercare
- Remove the needle using a smooth motion.
- Apply gentle pressure with gauze if needed.
- Dispose of the needle/syringe immediately in a sharps container.
What normal vs not-normal reactions look like
- Common: mild soreness, slight redness, or a small bump that improves over 24–48 hours.
- Concerning: worsening swelling, increasing heat, spreading redness, drainage, fever, or severe pain.
When these red flags appear, I recommend contacting your clinician rather than “waiting it out,” especially after a new site or a new batch of technique.
Troubleshooting: Pain, Bruising, Leaks, and Missed Doses
Even with good technique, reactions happen. Here’s how to think about them—objectively—so you can adjust intelligently next time.
If it hurts more than expected
- Double-check you’re using the subcutaneous route (not inadvertently going too deep).
- Rotate sites to reduce repeated irritation in one area.
- Avoid injecting into areas that are bruised, hard, or inflamed.
If bruising happens repeatedly
- Apply firm, gentle pressure after needle removal for the time your clinician advises.
- Ensure the skin fold is consistent (SC injections are sensitive to depth placement).
- If you’re on medications that affect bleeding, mention that to your prescriber—this changes what “normal bruising” means.
If you notice wetness or “leak”
Sometimes a small amount of fluid can appear at the site if placement or timing is off. If this is frequent, ask your clinician or nurse for an updated technique review—this is usually fixable with minor adjustments in angle, depth, or needle handling.
If you miss a dose
Don’t guess. Follow your prescriber’s written instructions or medication schedule guidance. In my experience, the safest approach is to follow the plan you were given rather than improvising.
When to Ask About Intramuscular (IM) Injections Instead
If your prescription says intramuscular, your injection plan should reflect that. There are also situations where patients benefit from refresher training because route affects both comfort and administration technique.
Reasons IM might be recommended
- Your prescriber specifically directed IM delivery for your product and plan.
- SC is causing persistent issues like significant site reactions (after ruling out technique problems).
- You have clinical circumstances that your clinician associates with IM use.
How to approach the decision responsibly
Don’t self-switch routes. Instead, bring your question back to your clinician: “My prescription is for B12—can you confirm SC vs IM for my exact dose and product?” In my practice, that single confirmation prevented weeks of trial-and-error.
FAQ
Is a vitamin B12 injection subcutaneous or intramuscular—how do I know which one I should use?
Use the route stated on your prescription or the route you were trained to perform. Subcutaneous and intramuscular injections differ in placement depth and angle, so switching without guidance can increase discomfort or cause inconsistent outcomes.
What’s the best subcutaneous site for vitamin B12 injections?
Common SC sites include the abdomen (avoiding the belly button area) and the thigh. The “best” site is often the one you can inject comfortably while rotating locations and avoiding irritated, bruised, or hardened skin.
How can I reduce soreness after a subcutaneous vitamin B12 injection?
Rotate sites, inject with steady control, let the alcohol swab dry before injecting, and apply gentle pressure afterward. Mild soreness is usually expected, but worsening redness, heat, swelling, or drainage should be evaluated by your clinician.
Conclusion
Performing a subcutaneous vitamin B12 injection well comes down to the fundamentals: correct route (vitamin b12 injection subcutaneous or intramuscular per your prescription), accurate site selection, clean technique, and a consistent workflow. In my hands-on experience, patients who focus on depth placement and site rotation usually see fewer bruises and less soreness over time.
Next step: Write down (1) your exact dose, (2) your prescribed route (SC or IM), and (3) your next injection site plan, then practice the process with a clinician’s instructions or training video until your steps feel repeatable.
Discussion