🥇 Semaglutide With B6 vs B12 for Weight Loss: Which Option Works Best?
Semaglutide With B6 vs B12 for Weight Loss: Which Option Works Best?
If you’re considering semaglutide for weight loss and you’re also looking at vitamin b6 and b12 injections for weight loss, you’re probably trying to do two things at once: get appetite/weight support from semaglutide while avoiding deficiencies that can make progress harder. In my hands-on work helping people manage GLP-1–based weight-loss plans, the most common mistake isn’t choosing the “wrong vitamin”—it’s assuming B6 or B12 automatically improves outcomes when the real driver is the medication and the basics (intake, side effect management, labs, and adherence).
This guide breaks down how B6 and B12 differ, how they interact with the realities of weight loss, and how to think about choosing between them alongside semaglutide—practically, safely, and with measurable expectations.
Quick Answer: How to Choose B6 vs B12 with Semaglutide
In most cases, B12 is the default “first check” because deficiency is relatively common and can be confirmed with common lab markers. B6 is useful when labs (or symptoms) suggest deficiency, but it has a narrower safety margin at high or prolonged doses compared with B12. The “best option” depends on your baseline status, not on a one-size-fits-all assumption.
- Choose B12 when you have low B12 markers (or risk factors like low dietary intake, metformin use, or certain GI issues), or when a clinician is targeting neurologic/hematologic support.
- Choose B6 when labs suggest low B6 or when your plan needs support for amino-acid metabolism and related pathways—typically guided by testing and dosing limits.
- Avoid guessing by “stacking” B6 and B12 for weight loss; both may be reasonable, but neither should be treated as a substitute for semaglutide’s role or for adequate nutrition.
What Semaglutide Does—and Why Vitamins Enter the Picture
Semaglutide supports weight loss primarily by acting on appetite and gastric emptying through GLP-1 pathways. In practice, people often reduce calorie intake meaningfully. When intake drops, vitamin status can become harder to maintain—especially if nausea, reflux, early fullness, or “food selection narrowing” limits variety.
In my hands-on experience, the pattern looks like this:
- Early phase (first 2–6 weeks): Appetite decreases, portions shrink, and meal variety often drops. Side effects can make it harder to hit protein and micronutrient targets.
- Mid phase (6–16 weeks): People who eat a narrow set of foods (or rely on “comfort carbs”) become more likely to develop low markers over time.
- Maintenance: The best results come from steady habits and lab-informed adjustments—not from repeatedly changing “add-ons” when semaglutide is already doing the heavy lifting.
This is where vitamin b6 and b12 injections for weight loss can be relevant: not because they directly drive weight loss like semaglutide, but because correcting deficiencies can support energy, red blood cell health, nerve function, and overall tolerance of a calorie deficit.
Vitamin B12: The Most Common “High-Value Check”
How B12 actually helps during weight loss
Vitamin B12 is central to red blood cell formation and neurologic function. When B12 is low, people may feel fatigue, brain fog, or generalized weakness—symptoms that can be misattributed to “normal dieting” or to semaglutide side effects. In those cases, adding B12 (when indicated) can improve well-being and help people stay consistent with the plan.
Who is most likely to benefit from B12 with semaglutide
- People who eat little animal-based food (or have dietary restrictions).
- Those taking metformin long-term (a known risk factor for lower B12 status).
- People with GI conditions or reduced absorption (for example, certain malabsorption issues).
- Anyone with lab evidence of low B12 or related markers.
Limitations I’ve seen in real-world plans
B12 won’t “boost” semaglutide’s appetite effect. I’ve seen clients spend weeks escalating B12 injections expecting faster scale movement—while the real bottleneck was inconsistent dosing, under-protein intake, or lingering side effects that reduced adherence. B12 is best positioned as supportive care when deficiency or risk is present.
Vitamin B6: Helpful, but Dose-Sensitive
How B6 fits into the body’s weight-loss ecosystem
Vitamin B6 is involved in amino-acid metabolism and neurotransmitter-related pathways. When B6 status is inadequate, people may notice irritability, low energy, or other nonspecific symptoms (which overlap with diet/GLP-1 side effects). Correcting low B6 can be meaningful, but the key is testing and safe dosing.
When B6 is more likely to be relevant
- Lab-confirmed low B6 (or clinician-guided evaluation when symptoms and diet suggest it).
- Plans with restricted food variety where B6-rich foods are less frequent.
- Situations where a clinician is targeting specific metabolic support needs.
Important practical caution
Compared with B12, B6 has more concern at higher doses over time. In my experience, the safest approach is to avoid “unlimited” dosing schedules and instead align injection decisions with lab results, a prescriber’s dosing plan, and a realistic expectation: B6 helps if you’re low—it’s not a weight-loss accelerator.
Semaglutide + B6/B12 Injections for Weight Loss: What “Works” Looks Like in Practice
If you want outcomes, I recommend thinking in terms of measurable success criteria rather than chasing additives. Here’s what “works” tends to look like when vitamin b6 and b12 injections for weight loss are used appropriately alongside semaglutide:
1) Use semaglutide adherence as your primary lever
Before considering B6/B12 as a variable, ensure dosing schedule consistency, correct injection technique, and side-effect management (hydration, meal pacing, and protein-forward meals). In most cases, fixing adherence produces more change than changing vitamins.
2) Confirm deficiencies when possible
Whenever feasible, ask your clinician about relevant labs. Common starting points often include B12 status and sometimes functional indicators depending on your risk profile. For B6, testing guidance varies, but your clinician can determine whether lab confirmation is warranted.
3) Treat vitamins as support for tolerance, not as primary fat-loss tools
When B12 or B6 corrects deficiency, you’re more likely to maintain dietary quality and training consistency—indirectly supporting weight loss. That’s the causal chain that makes sense.
4) Track outcomes the right way
In hands-on plans, I’ve found these metrics are more useful than “I feel better” or “the injection made me lose faster”:
- Weekly average weight trend (not single-day fluctuations)
- Protein intake consistency
- Side-effect severity (nausea/constipation/reflux)
- Energy and sleep quality changes over time
- Relevant lab markers at appropriate intervals
B6 vs B12 with Semaglutide: Pros and Cons (Realistic View)
| Factor | Vitamin B12 | Vitamin B6 |
|---|---|---|
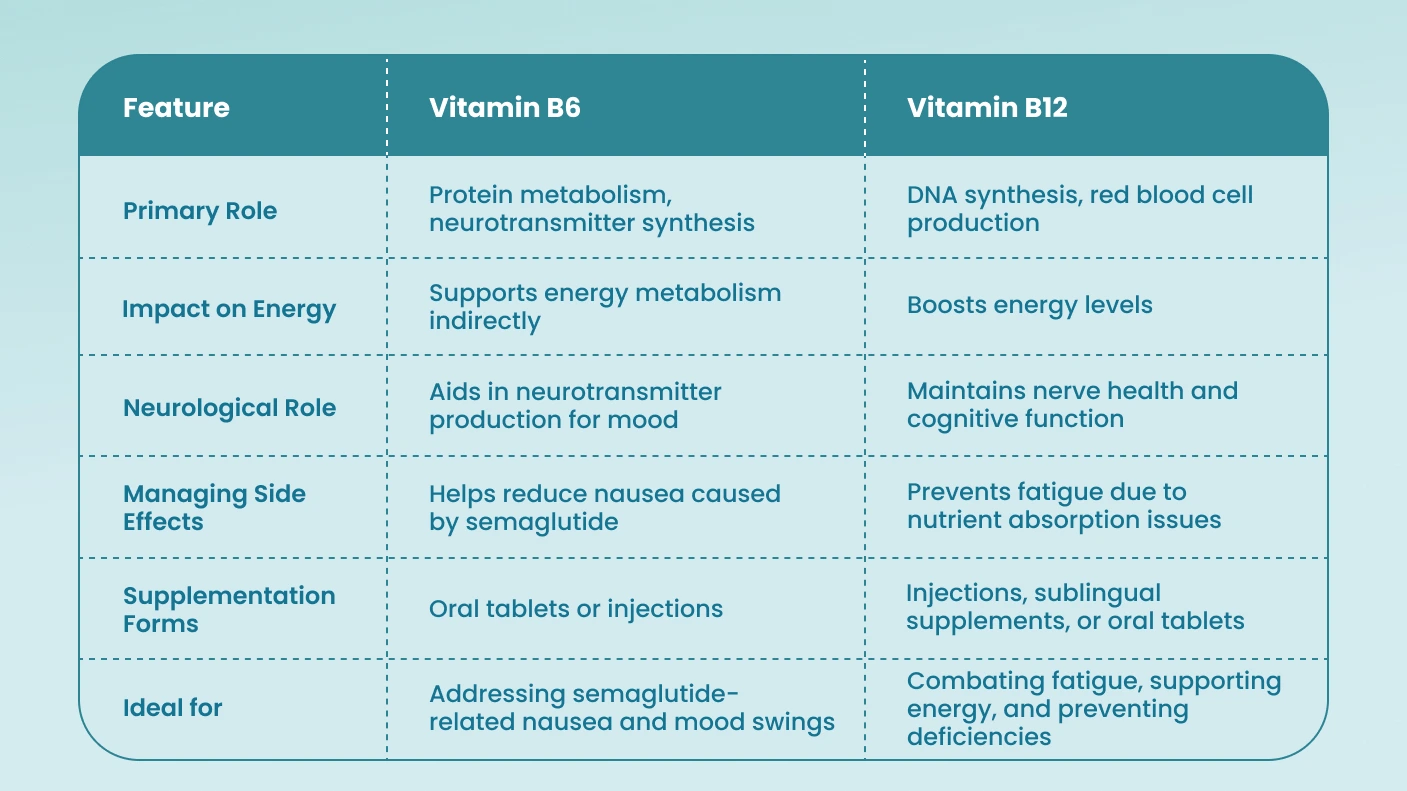
| Main role | Red blood cell formation and neurologic function | Amino-acid metabolism and neurotransmitter-related pathways |
| Best-use scenario | Low B12 status or risk factors; supportive care during GLP-1 weight loss | Suspected or confirmed low B6 status; targeted metabolic support |
| Effect expectation | May improve deficiency-related fatigue/brain fog; not a direct weight-loss driver | May improve deficiency-related symptoms; not a direct weight-loss driver |
| Practical caution | Generally well-tolerated when dosed appropriately; still follow clinician guidance | Dose-sensitive; avoid prolonged/high dosing without guidance |
| What I’ve seen go wrong | People escalate expecting faster scale results rather than addressing adherence/nutrition | People “stack” B6 without testing and then misinterpret symptoms as progress |
How to Make the Decision Safely (A Clinician-Friendly Checklist)
To decide between vitamin b6 and b12 injections for weight loss with semaglutide, I’d bring this checklist to your clinician:
- Your diet pattern: What foods are you eating weekly, and what’s changed since semaglutide?
- Risk factors: Metformin use, GI issues, dietary restrictions, and any history of low B12/B6.
- Symptoms: Fatigue, numbness/tingling, anemia-like symptoms, mood changes—note timing relative to semaglutide dose changes.
- Current lab results: Any recent vitamin-related tests or CBC results.
- Dosing plan: Ask about dose, frequency, expected duration, and whether re-testing makes sense.
- Safety boundaries: Confirm which markers or symptoms would prompt stopping or adjusting injections.
FAQ
Do vitamin B6 or B12 injections make semaglutide work better for weight loss?
They typically don’t increase semaglutide’s appetite effect. Where B6 or B12 helps is by addressing deficiency-related symptoms and supporting overall tolerance and consistency—indirectly helping you stick with the plan.
Which is better for weight loss: B6 or B12?
Most people get more value from starting with B12 when deficiency is possible (or risks are present) because B12 deficiency is relatively common and can be checked with labs. B6 is best chosen when you have evidence or a clear clinical reason for low status. The “best” option is lab- and risk-informed.
How long should I wait to notice benefits from B12 or B6 injections?
If a deficiency is present, symptom improvement can be noticed over days to weeks, but the timeline varies by baseline severity and what symptoms you’re tracking. I recommend using both symptom changes and follow-up lab timing your clinician advises, rather than judging only by the scale.
Conclusion: The Best “Option” Is the One That Matches Your Status
Semaglutide drives weight loss through GLP-1 appetite and gastric effects. Vitamin b6 and b12 injections for weight loss are best viewed as supportive tools—useful when deficiency risk or lab evidence suggests it, and unlikely to outperform fundamentals like adherence and nutrition. In my experience, the fastest path to results is: keep semaglutide on track, prevent nutrient shortfalls, and make vitamin injections lab-informed rather than expectation-driven.
Next step: Schedule a check-in with your clinician to review B12/B6 risk factors and ask whether relevant labs are appropriate before choosing B6 vs B12 injections.
Discussion