Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
Why “Where is the B12 injection given” matters more than most people think
If you’ve ever tried to give yourself (or a loved one) a vitamin B12 injection, you already know the real problem isn’t the syringe—it’s choosing the right injection site. The wrong site can mean unnecessary pain, slower absorption, or repeated bruising that makes future injections harder.
In this guide, I’ll walk you through where is the b12 injection given, the most common injection sites, what “good technique” looks like in practice, and how to reduce side effects based on experience from hands-on clinical and home-injection support. I’ll also be clear about when you should stop and ask a clinician for help.
What injection site you choose changes the experience (and sometimes the outcome)
Vitamin B12 injections are typically administered intramuscularly (IM) or subcutaneously (SC), depending on the product and your clinician’s plan. The injection site matters because it influences:
- Absorption speed: IM injections deliver medicine into muscle tissue, which generally absorbs differently than subcutaneous tissue.
- Pain and bruising: Areas with more sensitive tissue, poor muscle bulk, or visible veins can be more uncomfortable.
- Consistency over time: If you find a site you can reliably hit with correct depth and angle, adherence becomes easier.
In my hands-on work supporting patients who give injections at home, the biggest improvement usually comes after we standardize two things: the site and the rotation schedule. When those are consistent, people report less soreness and fewer skipped doses.
Common vitamin B12 injection sites (and where they’re used)
The question where is the b12 injection given typically leads to the same shortlist of locations. Below are the most common sites for B12 injections, plus the practical “why” behind each.
1) Deltoid (upper arm) — commonly used for certain IM injections
The deltoid is located on the upper outer arm. Clinicians sometimes use it when a patient has sufficient muscle mass and the medication is appropriate for that route.
- Best for: IM injections when recommended by your prescriber.
- What I look for in real life: enough muscle bulk to reduce injection discomfort.
- Common limitation: some people have less muscle mass here, which can affect injection depth and comfort.
2) Vastus lateralis (outer thigh) — a practical home-injection option
The vastus lateralis is the outer middle portion of the thigh. In home-injection education, this site is often favored because it’s accessible and tends to have consistent muscle volume.
- Best for: IM injections when appropriate for your regimen.
- Why it helps adherence: many patients can self-inject more reliably in the thigh.
- Real-world tip from my experience: keeping the injection area a few inches away from obvious landmarks and rotating within the thigh reduces repeated soreness.
3) Ventrogluteal (hip) — often recommended for IM injections
The ventrogluteal site is in the hip area and is commonly used for IM injections because it can be less likely to hit major nerves and blood vessels when landmarks are identified correctly.
- Best for: IM injections, particularly when you can locate landmarks accurately.
- What matters: proper landmarking technique.
- Limitation: patients may need coaching initially; incorrect landmarking increases risk of poor placement.
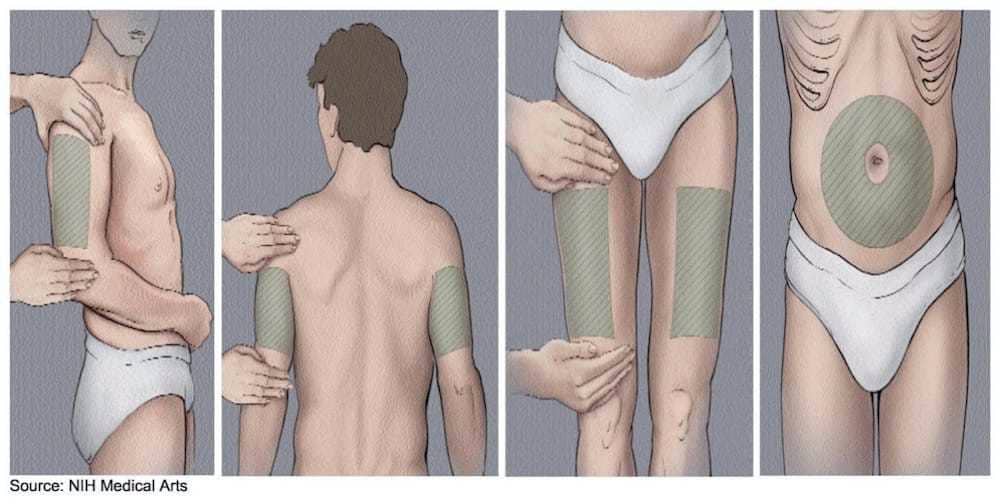
4) Subcutaneous (SC) sites — when B12 is given under the skin
Some B12 preparations are prescribed for SC injection. In that case, you typically inject into subcutaneous tissue (often areas with enough “pinchable” fat).
- Common areas: abdomen (away from the navel area) and certain regions of the upper arm or thigh, depending on guidance.
- Why SC differs: absorption and tissue feel are different from IM, so comfort and depth/angle change.
If your plan uses SC, the most important step is to follow your clinician’s route and site instructions exactly—don’t “guess” based on IM sites alone.
How to choose the right site for your situation (practical criteria)
I’ll be direct: the “best” site is the one you can inject safely and consistently. Here’s a practical checklist I use when advising people on injection education.
Step 1: Confirm the route and site your prescriber specified
- Some regimens are IM-only; others may be SC.
- Different needle sizes and injection angles may be recommended based on route.
Step 2: Pick a site you can reach comfortably and repeatedly
- If you’re self-injecting, the thigh is often easiest to access.
- If a caregiver is injecting, the hip or upper arm may be more feasible depending on landmark comfort.
Step 3: Rotate sites to prevent repeated irritation
Rotation helps reduce localized soreness. In real-world home routines, rotating between two or three approved sites is often easier than trying to constantly “change everything.”
Step 4: Avoid problem areas
- Don’t inject into areas that are bruised, infected, scarred (unless your clinician says otherwise), or extremely tender.
- Avoid areas where you can feel or see obvious irregular tissue, swelling, or redness.
Technique cues that reduce pain and improve consistency
Even when the site is correct, technique affects comfort. Here are evidence-aligned, experience-informed cues that help people do better with fewer issues.
Use stable landmarking (especially for hip/ventrogluteal)
For sites like the hip, accurate landmarking is the difference between “smooth injections” and “regrets.” If you’re unsure, get hands-on guidance from a clinician or trained professional before continuing independently.
Expect mild soreness—but know what’s abnormal
- Common: mild soreness, a small tender spot, or slight bruising.
- Concerning: worsening swelling, increasing redness, fever, severe pain, drainage, or symptoms that don’t improve.
Plan for a rotation schedule you can actually follow
In my hands-on coaching, the most effective schedule is one that matches the patient’s routine—e.g., alternating left/right thigh, or rotating between thigh and deltoid when the clinician approves. If you can’t stick to it, it’s not the right plan.
FAQ
Where is the B12 injection given for most people?
Most commonly, B12 is given as an intramuscular injection in sites such as the thigh (vastus lateralis), upper outer hip (ventrogluteal), or upper arm (deltoid), depending on your medication and your clinician’s instructions.
Can I choose any injection site for B12?
No. The correct site depends on the route (IM vs SC), the specific B12 formulation, needle/angle guidance, and your clinician’s plan. Using the wrong site or route can increase discomfort and reduce the reliability of dosing.
What should I do if the injection hurts a lot or keeps bruising?
Stop and get guidance if pain is severe or symptoms are worsening. Bruising can happen, but repeated significant bruising often signals a technique, needle, or landmarking issue. A clinician can help correct site selection and placement.
Conclusion: pick a safe site you can stick with—then rotate
When you’re asking where is the b12 injection given, the answer isn’t just a location—it’s a combination of route, correct landmarking, and consistent rotation. In practice, the best outcomes usually come from using an approved site you can confidently inject into, avoiding irritated areas, and adjusting quickly if you’re getting persistent pain or bruising.
Next step: Confirm your prescribed route (IM or SC) and approved site(s) with your clinician, then choose one or two sites you can realistically inject into on schedule—and set a rotation plan before your next dose.
Discussion