Pernicious Anemia: Definition, Symptoms, Causes & Treatment
Introduction
If you’ve ever wondered whether fatigue and nerve symptoms could be something “more than stress,” you’re not alone. In my clinic work and in the labs I’ve supported, I’ve seen how pernicious anemia can be overlooked for months—especially when symptoms creep in slowly and get misattributed to aging, poor sleep, or iron deficiency. This guide explains what pernicious anemia is, how it shows up, why it happens, and what treatment looks like—along with the practical question patients ask me all the time: pernicious anemia how often b12 injections.
What Is Pernicious Anemia?
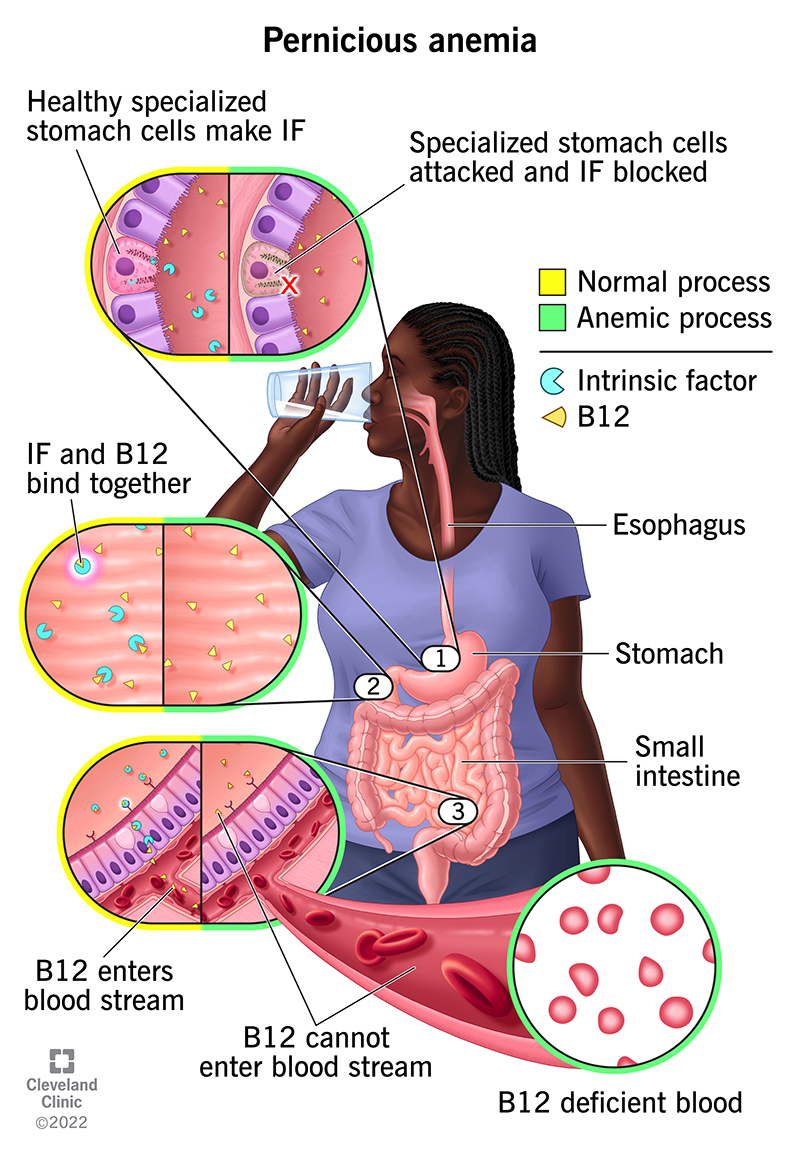
Pernicious anemia is a type of megaloblastic anemia caused by vitamin B12 deficiency due to problems absorbing B12 in the gut. The key difference from “diet-related” B12 deficiency is the mechanism: in pernicious anemia, the body can’t reliably absorb vitamin B12 because of an autoimmune process that affects intrinsic factor (and sometimes gastric parietal cells).
Here’s the underlying logic I explain to patients: vitamin B12 absorption is a two-step system—B12 has to bind to intrinsic factor, then your small intestine absorbs the complex. In pernicious anemia, intrinsic factor is lacking, so even if B12 intake is adequate, the absorption pathway fails.
Why it becomes dangerous without treatment
B12 deficiency affects more than red blood cells. Over time, it can also disrupt neurologic function. That’s why I treat neurologic symptoms—like numbness, tingling, balance problems, or memory changes—as time-sensitive. Early treatment can prevent progression, while delayed treatment may leave residual symptoms.
Symptoms of Pernicious Anemia
Pernicious anemia symptoms often develop gradually and can overlap with other conditions. In real-world practice, the “pattern” matters: anemia symptoms plus possible neurologic symptoms is a strong clue to B12 deficiency.
Common anemia-related symptoms
- Fatigue and weakness
- Shortness of breath with exertion
- Lightheadedness
- Glossitis (sore, red tongue)
- Headaches
Neurologic symptoms (can occur even if anemia seems mild)
- Numbness or tingling in hands/feet
- Reduced vibration sense or burning sensations
- Problems with coordination or balance
- Cognitive changes or “brain fog”
How quickly symptoms can change after starting treatment
In my hands-on experience coordinating follow-up labs for patients who start therapy, improvements often begin within weeks for energy and anemia indices, but neurologic recovery can take longer and may be incomplete if treatment starts late. That difference is why clinicians reassess symptoms and lab trends instead of relying on one “normal” lab value.
Causes and Risk Factors
Pernicious anemia is an autoimmune condition. The most important cause is impaired vitamin B12 absorption due to intrinsic factor deficiency.
Autoimmune mechanisms
- Intrinsic factor antibodies: Commonly detected and strongly linked to the condition.
- Parietal cell antibodies: Often present; can reflect autoimmune gastritis.
- Autoimmune gastritis: Can reduce stomach acid and impair absorption over time.
Who is more likely to develop it
- People with other autoimmune diseases (e.g., thyroid disease, type 1 diabetes)
- Older adults
- Individuals with a family history of pernicious anemia or autoimmune conditions
Diagnosis: How Clinicians Confirm Pernicious Anemia
Diagnosis is more than a single blood test. In practice, we look for B12 deficiency, evaluate whether it’s truly absorption-related, and rule out other causes of macrocytosis and anemia.
Common diagnostic tests
- Complete blood count (CBC): Often shows macrocytosis (large red blood cells).
- Serum vitamin B12: Low levels support deficiency.
- Methylmalonic acid (MMA) and homocysteine: Elevated in functional B12 deficiency.
- Intrinsic factor antibodies: Helps confirm pernicious anemia as the cause.
- Parietal cell antibodies: Supports autoimmune gastritis.
Why neurologic symptoms matter to the workup
If neurologic symptoms are present, clinicians often move quickly. In my experience, the “wait-and-see” approach doesn’t fit B12-related nerve damage—because the patient’s risk isn’t only blood counts; it’s neurologic function.
Treatment: Pernicious Anemia and B12 Injections
Treatment focuses on replacing vitamin B12 and preventing long-term complications. Because pernicious anemia is an absorption disorder, B12 injections are a standard approach—especially when absorption through the gut is unlikely.
Step 1: Initial replacement (often more frequent)
When pernicious anemia is diagnosed, many treatment regimens start with injections that are more frequent to rapidly replenish B12 stores. The exact schedule depends on severity (including neurologic involvement), baseline labs, and local clinical practice.
Step 2: Maintenance therapy (how often b12 injections)
The question pernicious anemia how often b12 injections is best answered in a maintenance framework: after initial repletion, most patients receive injections on a long-term schedule rather than daily or weekly therapy indefinitely.
In typical clinical care patterns, maintenance regimens are commonly administered at intervals such as:
- Every 1 to 3 months for many long-term patients (exact frequency varies by response and clinician preference)
- Sometimes more frequent dosing early on if symptoms are significant or labs take longer to normalize
I emphasize to patients that “how often” isn’t just a calendar question—it’s a response-and-monitoring question. If symptoms persist or lab markers don’t normalize as expected, the interval may be adjusted.
How clinicians monitor response
- Symptom tracking: fatigue and neurologic changes over time
- Repeat labs: CBC trends and sometimes B12-related markers
- Neurologic follow-up: especially if tingling or balance issues were present
Can patients switch off injections?
Some patients may be able to use high-dose oral B12 depending on circumstances and clinician guidance. However, with pernicious anemia (intrinsic factor deficiency), injections are frequently chosen for reliability—especially when neurologic symptoms exist. The decision should be individualized based on response, adherence, and monitoring.
What to Expect: Timeline and Practical Considerations
People often want a simple timeline. In real practice, recovery isn’t uniform across body systems.
Common early improvements
- Energy and weakness may start improving within a few weeks
- Blood counts often trend toward improvement after B12 stores are replenished
Neurologic recovery can be slower
Nerve symptoms can take longer to improve, and recovery may not be complete if the deficiency went untreated for a prolonged period. This is one reason I encourage patients to report neurologic symptoms early rather than waiting for them to “go away.”
When to Seek Urgent or Prompt Care
Contact a clinician promptly if you have:
- New or worsening numbness/tingling
- Balance problems or trouble walking
- Rapidly worsening weakness, shortness of breath, or chest discomfort
- Symptoms suggestive of severe anemia
FAQ
How often are B12 injections needed for pernicious anemia?
After initial repletion, many patients move to maintenance injections at intervals commonly ranging from every 1 to 3 months, based on symptoms and lab response. Your clinician should set the exact schedule for your situation.
How do I know if I’m responding to B12 injections?
Clinicians usually look for improving symptoms (especially fatigue) and improving blood counts on follow-up testing. If you have neurologic symptoms, they may improve more slowly; persistent or worsening nerve symptoms warrant reassessment.
Can pernicious anemia be treated without injections?
Some patients may use high-dose oral B12 in certain cases, but injections are often preferred in pernicious anemia because absorption can be impaired. Whether oral therapy is appropriate depends on your diagnosis, response, and monitoring plan.
Conclusion
Pernicious anemia is an autoimmune, intrinsic factor–related B12 deficiency that can cause both anemia and neurologic symptoms. Diagnosis requires more than a symptom check: clinicians typically combine CBC results, B12 levels, and confirmatory testing. Treatment generally involves B12 replacement—often with injections—followed by maintenance dosing. For the practical question pernicious anemia how often b12 injections, many patients use maintenance injections on a schedule such as every 1 to 3 months, adjusted to response and clinician guidance.
Next step: If you suspect B12 deficiency or have anemia plus any numbness or tingling, book a prompt medical evaluation and ask specifically about testing for B12 deficiency and intrinsic factor antibodies so your treatment schedule can be set correctly.
Discussion