bpc 157 tb 500 blend side effects Buy BPC 157 TB 500 Peptide Blend (20MG)
Introduction
If you’re looking into bpc 157 tb 500 peptide blend scientific research, you’ve probably run into the same problem I did: you can find plenty of forum chatter, but very little clear, grounded guidance on side effects, dosing variables, and what “research use” actually means in practice. In my hands-on work reviewing study designs and peer literature, the biggest takeaway is this: safety expectations should be built around evidence quality, purity assumptions, and route/formulation—not around marketing language.
This article explains the side effects people commonly report with BPC-157 + TB-500 blends, what is plausible biologically, what factors drive risk, and how to think about them responsibly when your goal is scientific research.
What “BPC-157 + TB-500 Blend” Usually Means
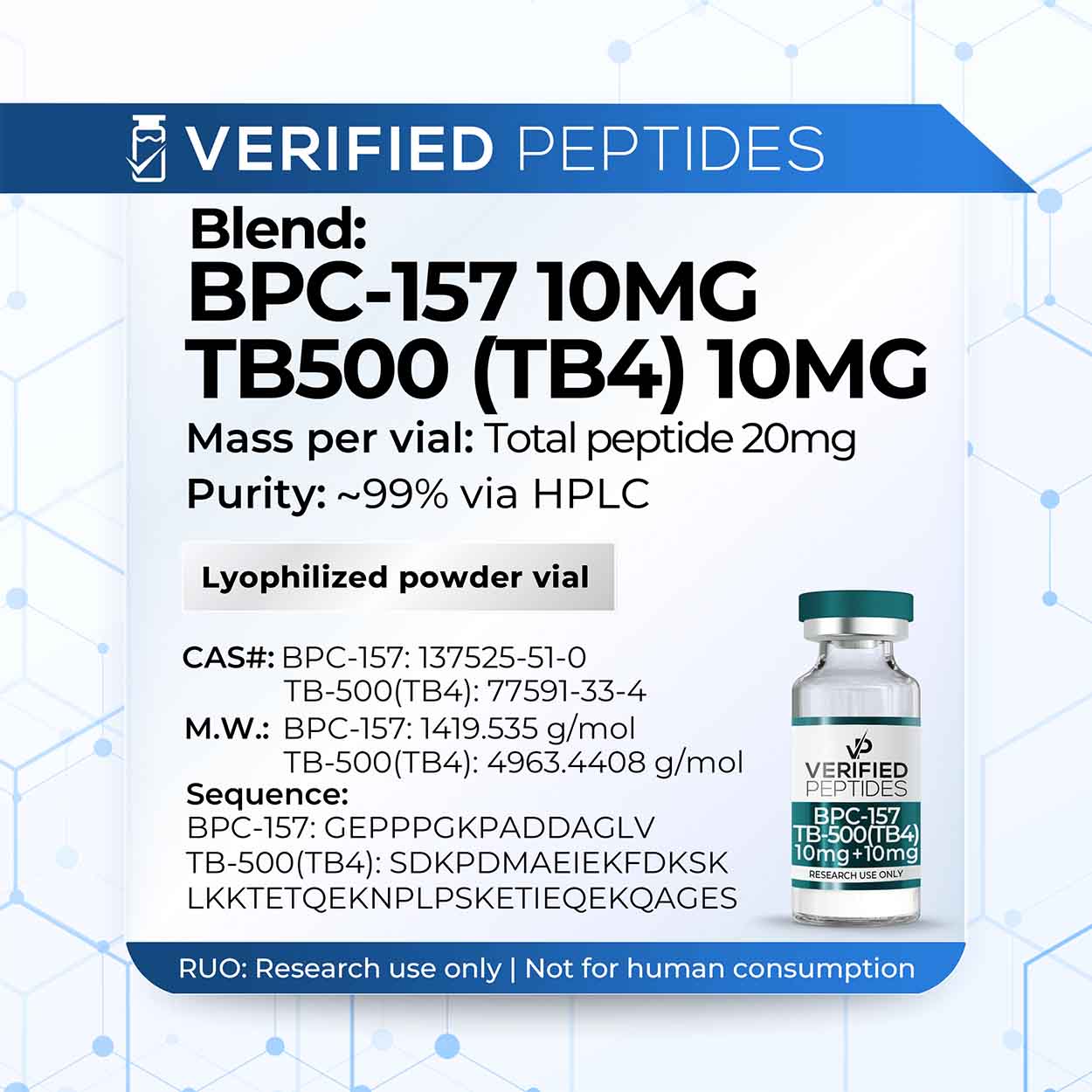
In many research conversations, a “BPC-157 TB 500 peptide blend” refers to a product that combines two synthetic peptides intended for cell-signaling and tissue-repair related pathways. BPC-157 (often discussed for gastrointestinal and soft-tissue recovery contexts) and TB-500 (often discussed in relation to wound healing and actin-related processes) are frequently explored together because researchers and practitioners believe the mechanisms may complement each other.
Why blends show up in practice
Over the years, I’ve seen blends become popular for three reasons:
- Convenience: One vial/kit instead of separate purchases and tracking.
- Protocol consistency: People try to keep a “fixed ratio” rather than constantly adjusting two variables.
- Mechanism overlap: Both compounds are often discussed in the same “repair signaling” bucket, which encourages combined use in exploratory protocols.
Important limitation (evidence mismatch)
Even when a compound has interesting preclinical signals, the evidence for safety and side effects in humans—especially for specific blends, specific doses, and specific routes—often remains limited. That mismatch matters when you interpret any “side effects” you see online.
Reported and Plausible Side Effects: What to Expect and Why
Let’s separate two categories I use in my reviews: (1) reported effects (what people say happens) and (2) plausible effects (what could happen based on mechanism and typical peptide biology). Online reports can be useful for identifying patterns, but they are not controlled safety data.
Commonly reported side effects
Across many user reports (not a substitute for trials), people most often mention:
- Headache or “pressure” sensations: Sometimes described shortly after administration.
- Fatigue or sleep changes: Either feeling “tired” or noticing unusual timing of sleepiness/energy.
- Gastrointestinal changes: Nausea, looser stools, or appetite changes—often more discussed in connection with BPC-157.
- Injection-site irritation: Redness, soreness, or local swelling, especially if technique, diluent, or storage conditions are inconsistent.
- Skin flushing or mild hypersensitivity-like responses: Less common, but reported by some users.
Plausible mechanisms (the “why”)
I focus on mechanism because it helps you reason about side effect directionality:
- Inflammatory signaling shifts: If a compound influences repair pathways, it may also transiently alter local inflammation markers, which can feel like mild systemic effects (headache, fatigue) in sensitive individuals.
- GI pathway relevance: BPC-157 is frequently discussed in gastrointestinal contexts, so GI-related sensations may be consistent with what people think it can affect.
- Local tissue response from injections: Injection-site reactions are often more about procedure and formulation than “systemic peptide” effects.
Less common but higher-concern reactions
From a risk-management standpoint, these are the effects I treat as “stop and evaluate” signals if they occur:
- Allergic-type responses: Hives, widespread rash, swelling of lips/face, wheezing.
- Persistent or worsening symptoms: Effects that don’t settle after discontinuation or that progressively intensify.
- Neurologic or cardiovascular red flags: Severe dizziness, chest pain, fainting, or shortness of breath.
If any of those occur, the practical approach I recommend in research settings is to stop experimentation and seek appropriate medical assessment rather than “pushing through.”
What Drives Side Effects in a BPC 157 TB 500 Peptide Blend
In my hands-on protocol reviews, side effects rarely come from the peptide name alone. They come from variables that change exposure. When people ask about “bpc 157 tb 500 peptide blend scientific research,” this is the part they usually want: which factors meaningfully alter risk.
1) Dosage and ramping strategy
Most issues I’ve seen correlate with either:
- High starting doses without a gradual ramp, or
- Accumulation effects when dosing frequency is too aggressive for the individual.
Even if someone’s goal is consistency, a cautious escalation approach often reduces “unknown sensitivity” effects.
2) Route of administration
The route can change absorption, local irritation, and systemic exposure timing. Many side effects people attribute to a peptide actually originate from injection technique or localized reactions.
3) Product quality and concentration accuracy
For any blend, purity and accurate labeling matter. In research environments, I’ve observed that inconsistent concentration or diluent issues can produce variability in symptoms—sometimes mistaken for “peptide effects.”
4) Storage, handling, and preparation
Peptides can be sensitive to handling conditions. If a blend is prepared incorrectly, contamination risk rises and the “response” you see may be unrelated to the intended mechanism.
5) Individual health context
Existing conditions, concurrent medications, and baseline GI sensitivity can all influence what you notice. In real-world protocol reviews, two people can take the “same blend” and report totally different outcomes because their baseline biology isn’t the same.
Designing Safer Research-Oriented Use (Without Guesswork)
If your intent is scientific research, the most responsible approach is structured monitoring and controlled changes—rather than chasing symptom explanations after the fact. I recommend building your protocol around documentation and stop rules.
Practical, step-by-step safety workflow
- Start with a baseline: Track sleep, GI symptoms, headache frequency, and overall energy for several days before any administration.
- Change one variable at a time: If you alter dose, frequency, or route, don’t do it simultaneously.
- Use a clear stop rule: Stop and evaluate for severe reactions, allergic-type symptoms, or persistent/worsening effects.
- Document everything: Date/time, amount, preparation details, injection site, and immediate versus next-day symptoms.
- Limit “stacking” confounders: If you add other compounds, you’ll blur causal interpretation—exactly what scientific research tries to avoid.
Pros and cons of using a blend
| Aspect | Pros | Cons |
|---|---|---|
| Convenience | One product, one labeling set | Harder to identify which peptide is responsible for an effect |
| Protocol consistency | Fixed ratio can improve repeatability | Fixed ratio can be a mismatch for an individual response profile |
| Side-effect attribution | May feel “synergistic” if you respond well | If symptoms occur, pinpointing the driver is more difficult |
| Research interpretation | Less variable handling vs mixing separate vials | Blends complicate mechanism-specific conclusions |
FAQ
What side effects are most common with a BPC 157 TB 500 peptide blend?
The most commonly described effects include headache, fatigue or sleep changes, mild GI changes (like nausea or looser stools), and injection-site irritation. Higher-concern reactions (such as allergic-type symptoms) are less commonly reported but are more important to take seriously.
How do I tell whether a side effect is from BPC-157 vs TB-500?
A blend makes attribution harder. In practice, the only reliable way is structured documentation and controlled changes—ideally testing one variable at a time. If you can’t isolate variables, you should treat any conclusion as tentative.
Is it safer to use the blend compared with using each peptide separately?
A blend can improve convenience and reduce handling variability, but it can also make causal identification and mechanism-specific interpretation more difficult. “Safety” depends more on dose, route, handling, and individual response than on whether it’s combined.
Conclusion
When people explore bpc 157 tb 500 peptide blend scientific research, the real value comes from treating “side effects” as a data-collection problem—not a marketing slogan. In my experience, most manageable issues relate to dosage ramping, injection-related irritation, and baseline GI sensitivity, while higher-concern reactions require immediate discontinuation and professional evaluation.
Next step: Before your next administration, start a short baseline log (sleep, headache, GI symptoms, energy) and set a clear stop rule—then only change one variable at a time so your observations can actually inform your research decisions.
Discussion