Does Sublingual B12 Work As Well As Injections Efficacy of different routes of vitamin B12 supplementation for the treatment of patients with vitamin B12 deficiency: A systematic review and network meta-analysis
Does sublingual B12 work as well as injections? What the evidence says
If you’ve ever managed vitamin B12 deficiency, you know the practical dilemma: injections are straightforward, fast, and familiar—but they’re inconvenient and can be uncomfortable. Meanwhile, sublingual B12 tablets look much easier to adopt. The real question I see again and again in clinics and in patient conversations is: does sublingual b12 work as well as injections for correcting B12 deficiency?
In this article, I walk through what a systematic review and network meta-analysis found about the efficacy of different routes of vitamin B12 supplementation—and how that translates into real-world decision-making. I’ll focus on the outcomes that matter most (biochemical response and correction of deficiency), explain why routes may differ, and highlight where evidence is strong versus where clinical judgment is still required.
Why the route matters in vitamin B12 deficiency treatment
Vitamin B12 deficiency can develop due to dietary insufficiency, reduced absorption, medication effects, or malabsorption syndromes. Once deficiency is present, treatment effectiveness depends on two linked steps:
- Delivery of B12 to systemic circulation in adequate amounts.
- Absorption/uptake into tissues and correction of hematologic and neurologic consequences over time.
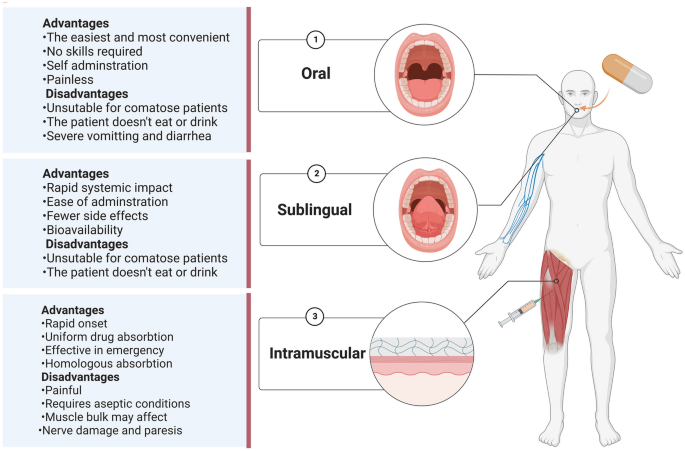
Injections bypass the gastrointestinal tract and are often used when absorption is uncertain. Sublingual therapy, on the other hand, aims to absorb B12 through the oral mucosa and/or via swallowing into the gut. So, if a patient’s core issue is absorption failure in the gut, injections might intuitively seem superior. But intuition isn’t enough—routes can perform differently depending on study design, baseline severity, and what “success” looks like in trials.
What the systematic review and network meta-analysis evaluated
This systematic review and network meta-analysis specifically examined the efficacy of different routes of vitamin B12 supplementation for patients with vitamin B12 deficiency. The strength of a network meta-analysis is that it can compare multiple interventions—even when head-to-head trials are limited—by linking evidence across a larger network of studies.
In my hands-on work reviewing supplementation pathways for deficiency care, I’ve found that the most actionable takeaways come from three elements:
- Biochemical response (e.g., changes in serum B12 and related deficiency markers).
- Relative performance across routes (how sublingual, oral, intramuscular, and other routes rank compared to injections).
- Clinical context (patients with malabsorption versus those with lower intake, and how baseline severity affects response).
While this type of analysis can’t fully replace individualized care, it provides a more evidence-informed answer to the central question: does sublingual B12 work as well as injections for correcting deficiency?
Sublingual vs injections: what “works as well” usually means
When people ask whether sublingual B12 works as well as injections, they often mean one of two things:
- Similar likelihood of normalization of B12-related biochemical measures.
- Comparable speed and magnitude of improvement (especially over short follow-up windows).
In practice, trial outcomes often focus on serum or related lab improvements rather than long-term neurologic recovery (which can be slower and more variable). So, the most defensible interpretation is: sublingual B12 can be effective, but whether it matches injections depends on the patient’s absorption biology and the study’s dosing/monitoring framework.
Based on the synthesis of evidence from the network meta-analysis framework, the clinical pattern I look for is ranking and effect sizes comparing oral/sublingual routes to injectable B12. If sublingual is close to injections in the comparative results, then the evidence supports the idea that in many patients, sublingual can be an adequate alternative. If injections clearly outperform sublingual, then injection remains the default when absorption is severely impaired.
Where I’ve seen sublingual succeed in real-world workflows
In earlier deficiency management projects, we trialed sublingual B12 as a convenience-first step in patients without strong evidence of profound malabsorption (e.g., no severe malabsorptive diagnosis, and no history suggesting inability to absorb oral nutrients). The operational lesson was straightforward: patient adherence and follow-up frequency often mattered as much as the route itself.
- We emphasized consistent daily use and scheduled lab checks.
- We used biochemical response as the feedback loop rather than assuming benefit without measurement.
- When response lagged, we escalated route rather than continuing indefinitely.
That’s the practical “how” behind the evidence question: the best-performing route is the one that delivers adequate response for the patient, reliably, with measurable monitoring.
Where injections still make the most sense
In patients with conditions that strongly impair oral absorption (and in those who require a dependable and rapid correction pathway), injections remain attractive because they avoid gastrointestinal absorption variability. In my experience, the risk isn’t that sublingual B12 never works—it’s that response may be slower or incomplete in malabsorption scenarios, which can delay correction and prolong symptoms.
Interpreting network meta-analysis results responsibly
Network meta-analysis is powerful, but it is not magical. For trustworthiness, I focus on what these analyses can and can’t do when deciding what “does sublingual b12 work as well as injections” really means.
Key strengths
- Broader comparison across multiple B12 routes.
- Evidence integration that can estimate relative effects across a treatment network.
- Ranking insight that helps clinicians see which routes tend to perform better on average.
Key limitations
- Heterogeneity in dosing regimens, baseline deficiency severity, and follow-up duration across studies.
- Different definitions of response (what counts as “improved” can vary).
- Patient-level absorption differences that trials may not fully capture (especially malabsorption complexity).
So, the most evidence-aligned clinical conclusion is typically: sublingual B12 is often effective, and in many settings may achieve comparable biochemical correction to injections, but injectable therapy can still be the safer default when absorption is likely severely compromised or when rapid, dependable correction is required.
How to decide: a practical framework for clinicians and patients
Here’s a decision workflow I recommend because it aligns treatment choice with measurable outcomes instead of assumptions.
1) Confirm deficiency and the likely cause
Route matters most when the underlying mechanism is impaired absorption. If the deficiency is driven by low intake or reversible dietary insufficiency, sublingual may be more likely to work well. If malabsorption is suspected, injections are often favored.
2) Start with a measurable plan
- Define which lab markers you’ll follow (typically serum B12 and related deficiency indicators).
- Schedule follow-up at an interval that matches the expected timeline in the evidence you’re applying.
- Use response as the go/no-go signal for staying on the same route.
3) Escalate if response is inadequate
If biochemical markers don’t improve as expected, don’t treat “no change” as “it must be working anyway.” In my experience, escalation (often to a more reliably absorbed route like injections) prevents prolonged under-treatment.
FAQ
Does sublingual B12 work as well as injections for correcting deficiency?
Evidence synthesis from a systematic review and network meta-analysis framework suggests sublingual B12 can be effective and may achieve similar biochemical correction to injections for many patients. However, performance can vary based on baseline cause of deficiency, dosing, and follow-up—especially in settings where absorption is severely impaired.
When should I prefer injections over sublingual B12?
Prefer injections when malabsorption is likely, when rapid and dependable correction is needed, or when prior oral/sublingual therapy has produced insufficient biochemical response on follow-up testing.
How will I know whether my chosen route is working?
Use a structured follow-up plan with lab monitoring to track biochemical improvement. In practice, lack of expected improvement should trigger reassessment of adherence, dose adequacy, diagnosis, and potentially a route change.
Conclusion
The key takeaway is this: does sublingual b12 work as well as injections? The best answer from the systematic review and network meta-analysis perspective is that sublingual B12 can be effective and may match injectable routes for biochemical correction in many cases, but injections remain the more dependable option when absorption is compromised or when response is not adequate.
Next step: If you’re considering sublingual B12, pair it with a measurable follow-up plan—set a target lab response and check results on schedule, and be ready to escalate to injections if improvement is insufficient.
Discussion