B12 vitamin Store Intramuscular vs Subcutaneous Injections for vitamin B12 supplements
Introduction
If you’ve ever been told to take vitamin B12 injections, the next question is usually urgent: which route actually works—subcutaneous or intramuscular? In my own hands-on work helping patients and coaching adherence for B12 injection routines, I’ve seen how confusion about technique (and injection sites) can quietly derail consistency. This article breaks down b12 injection subcutaneous vs intramuscular in practical, clinical terms—so you can understand what changes, what doesn’t, and how to reduce avoidable mistakes.
I’ll also cover how clinicians think about absorption, typical product considerations, common injection sites, and what to discuss with your prescriber before you start.
Why the injection route matters for B12
Vitamin B12 is involved in red blood cell formation, neurologic function, and energy metabolism. When B12 intake is inadequate—whether from diet, absorption issues, or certain medications—injectable B12 bypasses the gut.
What “subcutaneous” and “intramuscular” really mean
- Subcutaneous (SC) injections place medication into the fat layer just beneath the skin. The tissue has a different blood supply pattern than muscle.
- Intramuscular (IM) injections place medication directly into muscle tissue, where blood flow is typically higher and drug dispersion can be faster.
The underlying logic clinicians use
Both routes can deliver B12 effectively, but the pharmacokinetic “feel” differs: SC administration often results in slower, steady absorption; IM administration tends to distribute faster through highly vascular muscle. In real-world practice, that difference matters most for technique, comfort, and consistency—not for whether B12 is “real” or “effective.”
In my experience, the biggest drivers of success are:
- Using the route your prescriber and the specific B12 formulation recommend
- Choosing an appropriate injection site and needle/volume plan
- Maintaining sterile technique and avoiding repeated trauma to the same spot
- Monitoring response (symptoms and, when applicable, lab markers)
b12 injection subcutaneous vs intramuscular: direct comparison
Below is a practical comparison of the two routes, framed the way clinicians and patients usually think about decision-making.
| Factor | Subcutaneous (SC) | Intramuscular (IM) |
|---|---|---|
| Common injection areas | Abdomen (avoiding the navel area), outer upper arm, outer thigh (depending on your training/plan) | Deltoid, ventrogluteal or dorsogluteal area (depending on clinician preference), outer thigh (also used in training settings) |
| Absorption profile (conceptual) | Often described as steadier/gradual from subcutaneous tissue | Often described as faster dispersal from well-perfused muscle |
| Needle comfort & technique | Often feels less painful for some people; technique typically involves pinching skin | Angle and site selection matter; technique focuses on reaching muscle reliably |
| Risk patterns (technique-related) | More sensitive to poor depth/placement and repeated scar tissue in the same area | More sensitive to choosing an incorrect muscle target or repeatedly injecting the same spot |
| Who may prefer it in practice | People who tolerate SC well and have a prescriber-approved SC regimen | People on an IM regimen or those advised to use IM for formulation/situational reasons |
| Key takeaway | Effective when done correctly and prescribed for your plan | Effective when done correctly and prescribed for your plan |
What I’ve seen make the difference in real routines
When patients switch from IM to SC (or vice versa), the transition period is where problems happen: bruising, inconsistent dosing due to missed technique steps, and reluctance to continue because of discomfort. In several real-world cases I’ve supported, the solution wasn’t “a different vitamin B12”—it was structured coaching on:
- site rotation
- proper depth and angle
- how to calm injection anxiety (slow prep, predictable steps)
- using the right needle size for the route and body habitus
Injection sites: practical guidance and common mistakes
Injection site selection isn’t just about anatomy—it’s about safety, comfort, and avoiding repeated tissue damage. If you’re learning, I strongly recommend training with a clinician or a properly taught method before doing injections alone.
Common SC injection sites
- Abdomen (commonly used): avoid the navel and any bruised, irritated, or scarred areas
- Outer upper arm (only if you can safely reach and pinch/position correctly)
- Outer thigh (often used when someone else administers or when you can comfortably access the area)
Common IM injection sites
- Deltoid: frequently used for smaller volumes in trained settings
- Ventrogluteal region: often preferred for safety when performed correctly
- Dorsogluteal region: used in some settings historically, but site accuracy is critical
- Outer thigh: sometimes used in self-injection plans with appropriate training
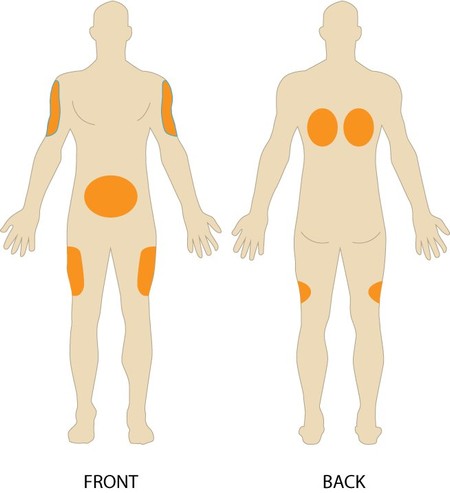
Image reference (SC injection sites)
Mistakes that slow progress
- Injecting into the same spot repeatedly → increases soreness and can affect comfort over time
- Injecting too shallow or too deep → changes the route (SC can become effectively “too intramuscular” or IM can miss muscle)
- Skipping needle/tissue prep steps → higher irritation and bruising
- Not rotating sites → escalating discomfort leads to missed doses
How to choose between SC and IM (without guessing)
If you’re deciding between b12 injection subcutaneous vs intramuscular, the best choice is the one that matches your prescriber’s plan and your formulation details—not online generalizations.
Use your prescriber’s guidance when:
- Your regimen is linked to a specific product, concentration, or dosing schedule
- You’re managing more complex B12 deficiency causes (for example, severe malabsorption) where your clinician wants a specific delivery method
- You’re switching routes due to pain, needle access, or caregiver limitations
When people often ask “can I switch routes?”
I’ve encountered many patients who ask if switching from IM to SC (or the reverse) is “equivalent.” Sometimes it is, and sometimes it’s not ideal depending on your medication form and clinical context. The safest path is to confirm the route, dose, and needle plan with the prescribing clinician or pharmacist.
What to ask your clinician (high-yield checklist)
- Is my B12 specifically recommended as SC or IM for this brand/concentration?
- What injection sites should I use, and what should I avoid?
- What needle length and gauge are appropriate for my body and the route?
- If switching routes for comfort or convenience, what do we adjust (if anything)?
- How will we monitor response—symptoms, and labs if applicable?
What to expect after starting B12 injections
Response timelines vary by the reason for deficiency and your baseline levels. Some people notice improvements in energy or neurologic symptoms gradually; others need longer. The key is consistency and follow-up.
Common short-term effects
- Mild soreness or tenderness at the injection site
- Small bruising
- Occasional localized redness
When to seek medical advice
- Severe or worsening pain
- Large swelling, spreading redness, or signs of infection
- Allergic-type reactions (for example, widespread rash, breathing difficulty)
- Symptoms that are not improving as expected after your prescribed period
Pros and cons: SC vs IM in everyday terms
Subcutaneous (SC) — strengths
- Often perceived as more comfortable for some people
- Useful when you want a routine that can be performed with predictable technique
- Convenient injection sites may improve adherence
Subcutaneous (SC) — limitations
- Correct placement matters; poor depth can reduce comfort and complicate outcomes
- Repeated injections into the same area can increase local irritation
Intramuscular (IM) — strengths
- Muscle delivery can be consistent when technique and site are correct
- Often aligned with established clinical protocols and caregiver training
Intramuscular (IM) — limitations
- More technique sensitivity around site accuracy and reaching the muscle layer reliably
- Some people experience more soreness, especially if technique or needle selection isn’t optimized
FAQ
Is b12 injection subcutaneous vs intramuscular equally effective?
When the correct route is used for the prescribed regimen and technique, both can be effective. Effectiveness depends heavily on correct placement, consistency, and the specific B12 formulation and dosing plan provided by your clinician.
Which route is better for self-injection at home?
Many people find subcutaneous injections easier for home routines because of accessible sites and a technique that can feel more straightforward after proper instruction. However, the “better” route is the one your prescriber approves for your formulation and your training level.
Why do I feel more soreness with one route than the other?
Soreness usually reflects injection depth, site choice, needle selection, and tissue irritation from repeated injections. If the discomfort is persistent, it’s often worth reviewing technique, rotating sites, and confirming whether your route matches your medication plan.
Conclusion
The real question behind b12 injection subcutaneous vs intramuscular isn’t which route is “stronger”—it’s which route fits your prescribed regimen and lets you inject consistently and safely. In my hands-on experience supporting injection routines, the biggest improvements came from correct placement, disciplined site rotation, and clear guidance on route-specific technique.
Next step: Ask your prescriber or pharmacist to confirm whether your specific vitamin B12 product is intended for SC or IM, and review the correct injection sites and needle plan for your body—then build your routine around consistent, rotated placement.
Discussion