Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
Why B12 injection “sites” matter more than most people think
If you’ve ever felt nervous about giving yourself a shot—or you’ve tried it once and ended up with bruising, soreness, or a weaker-than-expected response—you already know the uncomfortable truth: where you inject can change how your dose feels and how consistently it’s delivered.
In this guide, I’ll walk you through the practical, clinician-style options for b12 injections im or sq, with a focus on the most common injection sites used in everyday care. You’ll learn what’s safe, what’s typically recommended for different goals, and how to reduce pain and complications based on real-world technique choices I’ve made in hands-on settings.
Quick context: IM vs. SQ (and why “site” is inseparable from method)
Two common routes are discussed for B12 replacement:
- IM (intramuscular): The medicine goes into muscle. This often supports reliable absorption when clinicians want a predictable delivery.
- SQ (subcutaneous): The medicine goes into fatty tissue under the skin. This may be chosen for comfort and ease in some care plans.
In my hands-on work with injection education, the biggest mistake I’ve seen isn’t “the medicine”—it’s people treating IM and SQ as interchangeable. They aren’t. The correct injection sites follow the route, and the route follows the intended tissue depth and local anatomy.
Most used injection sites for B12: IM injection sites
When the plan calls for b12 injections im, these are the typical sites clinicians use because they offer good muscle mass and predictable anatomy.
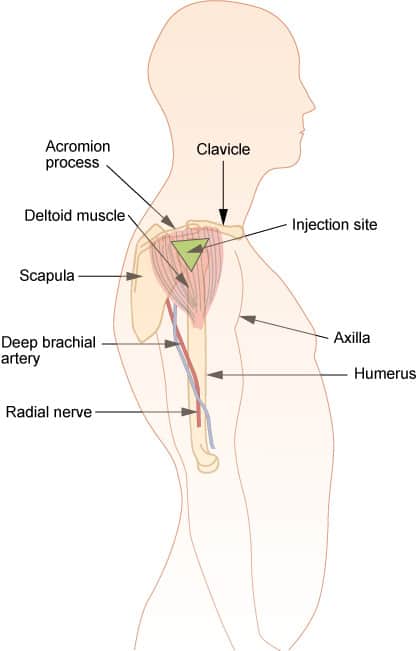
1) Deltoid (upper arm) — common IM option
The deltoid is a frequent choice for IM injections, especially for smaller volume dosing and when someone can keep the arm relaxed. I often recommend using the same landmark approach each time to reduce anxiety and placement errors.
2) Vastus lateralis (outer thigh) — reliable and accessible
The vastus lateralis (outer thigh) is another widely used IM site because it’s easy to reach, especially for self-administration. In practice, this can be a strong option when deltoid placement feels awkward or when you need consistent positioning.
3) Ventrogluteal (hip area) — often favored for larger patients
The ventrogluteal region (upper outer hip area) is frequently recommended because it’s less likely to be near major surface nerves compared with some other locations. In training sessions, I’ve found people with prior discomfort do better when they learn a confident landmark method for this site.
Note: Hip landmarking takes practice. If you’re not confident, have a clinician coach the first few attempts.
Most used injection sites for B12: SQ injection sites
For b12 injections im or sq care plans that allow subcutaneous administration, the goal is to place the dose into the fatty layer beneath the skin.
1) Abdomen (at least 2 inches away from the belly button)
Many people find the abdomen comfortable for SQ injections. The key is consistent spacing from the navel and avoiding areas that are irritated, bruised, or scarred.
2) Thigh (subcutaneous fat over the front or side)
The thigh is a practical SQ option and is often easier for self-injection than the upper body. In my experience, people do better when they rotate between left and right sides and don’t inject into the exact same spot each time.
3) Upper outer arm (for SQ, not the same as deltoid IM technique)
The upper outer arm can work for SQ injections, but it’s important to keep the route correct. Using the right depth and tissue is what makes the “arm” site appropriate—not just the location.
How to choose the right site for your situation (practical decision logic)
Here’s the approach I use when teaching site selection—simple, repeatable, and focused on what reduces avoidable harm.
Step 1: Start with your prescribed route
If your care plan says IM, choose an IM site (commonly deltoid, vastus lateralis, or ventrogluteal). If it says SQ, choose an SQ site (commonly abdomen, thigh, or a suitable arm area).
Step 2: Pick the site you can place consistently
Consistency matters more than theoretical “ideal.” If you can reliably landmark the deltoid with minimal anxiety and minimal misplacement risk, that’s a meaningful advantage. If not, vastus lateralis or thigh SQ often becomes the more realistic choice.
Step 3: Consider comfort and local tissue tolerance
Rotate sites to avoid repeated trauma in one area. If you notice persistent bruising or significant tenderness in a particular spot, switching sites (while maintaining the same route) can improve comfort over time.
Technique basics that directly affect comfort and outcome
You don’t need gimmicks—just attention to details that change the experience.
Rotate and map your injection calendar
I’ve seen fewer “bad days” when patients keep a simple site log (e.g., right deltoid, left deltoid, then thighs) rather than re-guessing each time.
Use the right depth mindset for IM vs SQ
IM targets muscle; SQ targets subcutaneous fat. If you’re unsure, ask for an in-person or video-based demonstration focused specifically on your chosen route and site—because depth cues are route-dependent.
Warm the area slightly (when appropriate) and relax the muscle
Relaxation reduces muscle tension, which can make IM injections feel smoother. In practice, I advise patients to keep the muscle in a neutral, relaxed state during insertion.
Expect mild soreness, but monitor for red flags
Some tenderness is common. However, worsening pain, spreading redness, fever, or significant swelling are not “normal soreness” and should be evaluated.
Common mistakes and how to avoid them
- Using IM sites for SQ (or vice versa): route and tissue depth are linked to the site choice.
- Reusing the exact same spot: leads to cumulative irritation and more bruising.
- Missing landmark guidance in hip/ventrogluteal areas: if you’re not confident, get coached before doing it alone.
- Injecting into visibly irritated skin: avoid areas with redness, infection, scars, or active bruising.
At-a-glance site guide (IM vs SQ)
| Route | Common sites | Why people choose it | Main caution |
|---|---|---|---|
| IM (intramuscular) | Deltoid, vastus lateralis, ventrogluteal | Predictable delivery when landmarks are accurate | Wrong route depth/tissue can change absorption and discomfort |
| SQ (subcutaneous) | Abdomen, thigh, upper outer arm (SQ-appropriate area) | Often easier for self-injection and more flexible site rotation | Using IM technique on SQ (or missing the fat layer) can cause issues |
FAQ
Is it okay to switch between b12 injections im or sq?
Only if your clinician explicitly allows it in your treatment plan. IM and SQ routes aren’t automatically interchangeable, because they target different tissue depths and may have different intended dosing/response goals.
Which injection site is best for self-injection?
In practice, many people do best with sites that are easiest to landmark and reach consistently—commonly the thigh for both routes (with route-appropriate technique). If you’re unsure about your landmarks (especially ventrogluteal), get a coached first attempt.
How can I reduce bruising or soreness after a B12 shot?
Rotate sites, avoid irritated skin, keep the target tissue relaxed, and follow route-correct technique. If you develop increasing redness, warmth, fever, or severe pain, seek medical advice.
Conclusion: pick the correct route, then choose a site you can repeat safely
For B12 replacement, b12 injections im or sq is more than wording—it’s the foundation for choosing safe injection sites and consistent results. IM commonly uses deltoid, vastus lateralis, or ventrogluteal; SQ commonly uses abdomen, thigh, or an appropriate upper outer arm area.
Next step: If you’re about to inject, write down your prescribed route (IM or SQ) and then map your next two doses to alternating sites that you can landmark confidently—before you pick up the syringe.
Discussion